Socioeconomic Impacts of LCD-Treated Drinking Water Distribution in an Urban Community of the Kathmandu Valley, Nepal

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
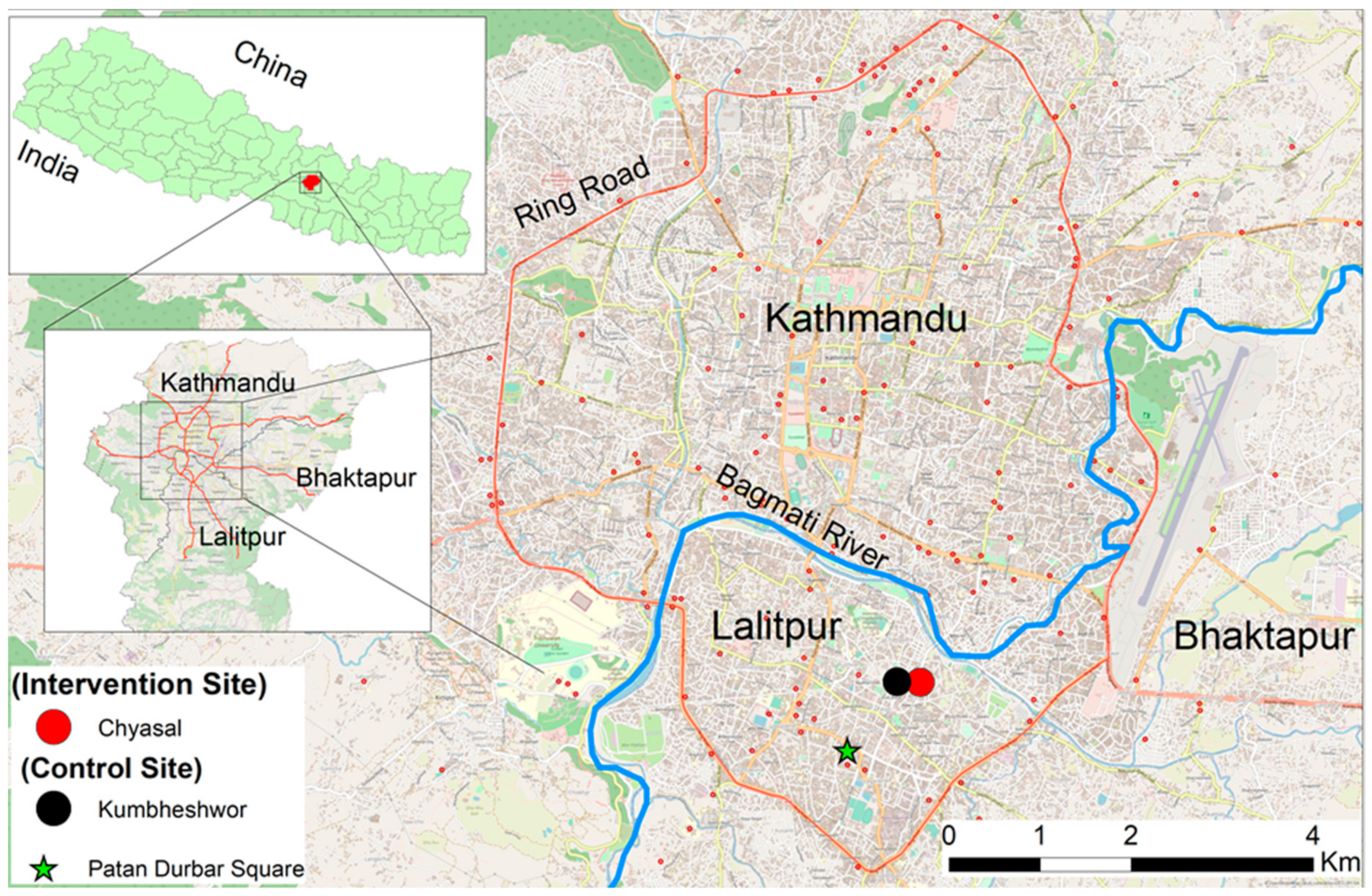
2.2. Study Area
2.3. LCD Water Treatment System
2.4. Intervention
2.5. Questionnaire Survey
- Sources of drinking water used: water source-wise percentage that households used for drinking.
- Water treatment practice: percentage of households that practiced water treatment.
- Quality perception of main source of drinking water: The quality perception of the main source of drinking water was measured by taste, smell, color, turbidity, and safety ranked as 1 (very poor or very unsafe); 2 (poor or unsafe); 3 (medium); 4 (good or safe); and 5 (very good or very safe). The quality perception was categorized as 1 good (very good and good) and 0 medium/poor (medium, poor and very poor) of each item.
- Water insecurity score (WIS): The water insecurity was measured by 15 defined statements on the negative perception of daily water use of a 6-point rating scale ranked as 1 (never); 2 (rarely); 3 (sometimes); 4 (often); 5 (mostly); and 6 (always). The WIS was calculated by averaging the scores of all statements of every household and was regarded as a continuous variable. A higher score indicated the high insecurity perception.
- Quality of Life (QoL): Questions from the World Health Organization quality of life-BREF were used to measure the QoL: 26 questions rated by 5-point scales—1 (very poor); 2 (poor); 3 (Neither poor nor good); 4 (good); and 5 (very good). After reversing the answers of three questions (question number 3, 4, and 26) according to the manual, the QoL score was calculated by averaging all questions values and was regarded as a continuous variable. Higher scores indicate a better QoL perception.
- 6.
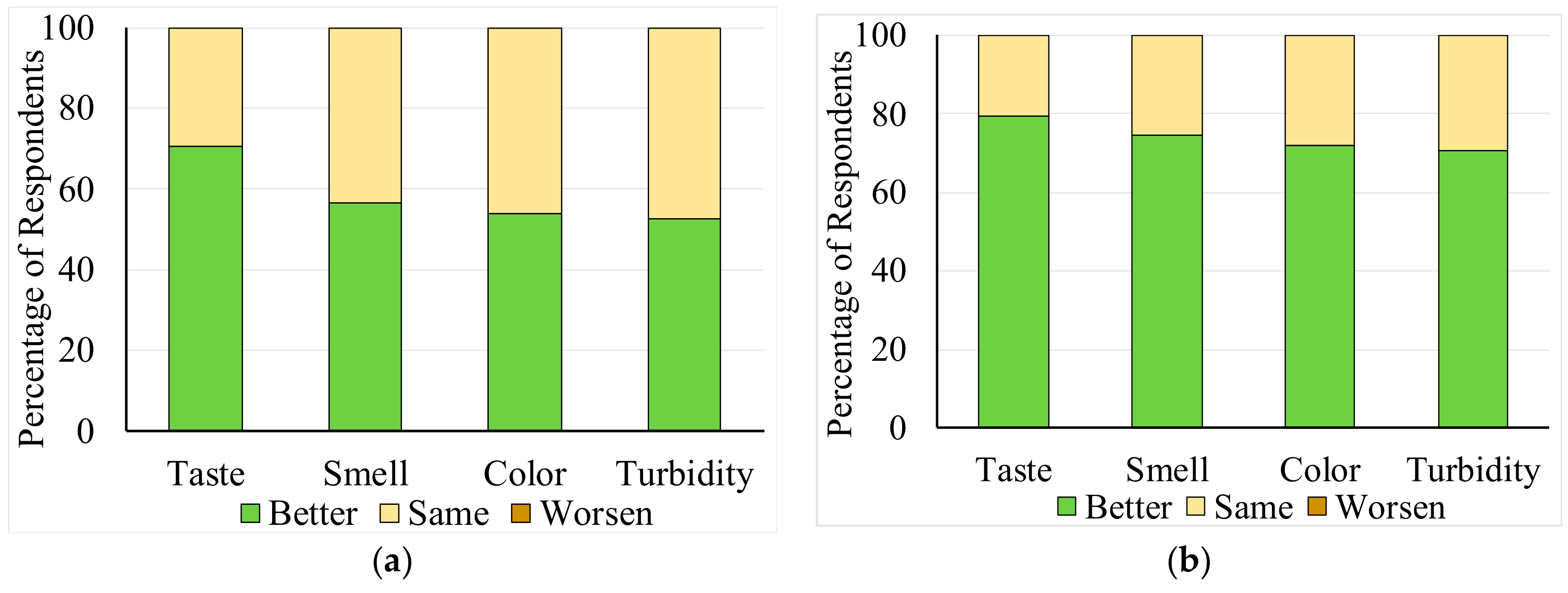
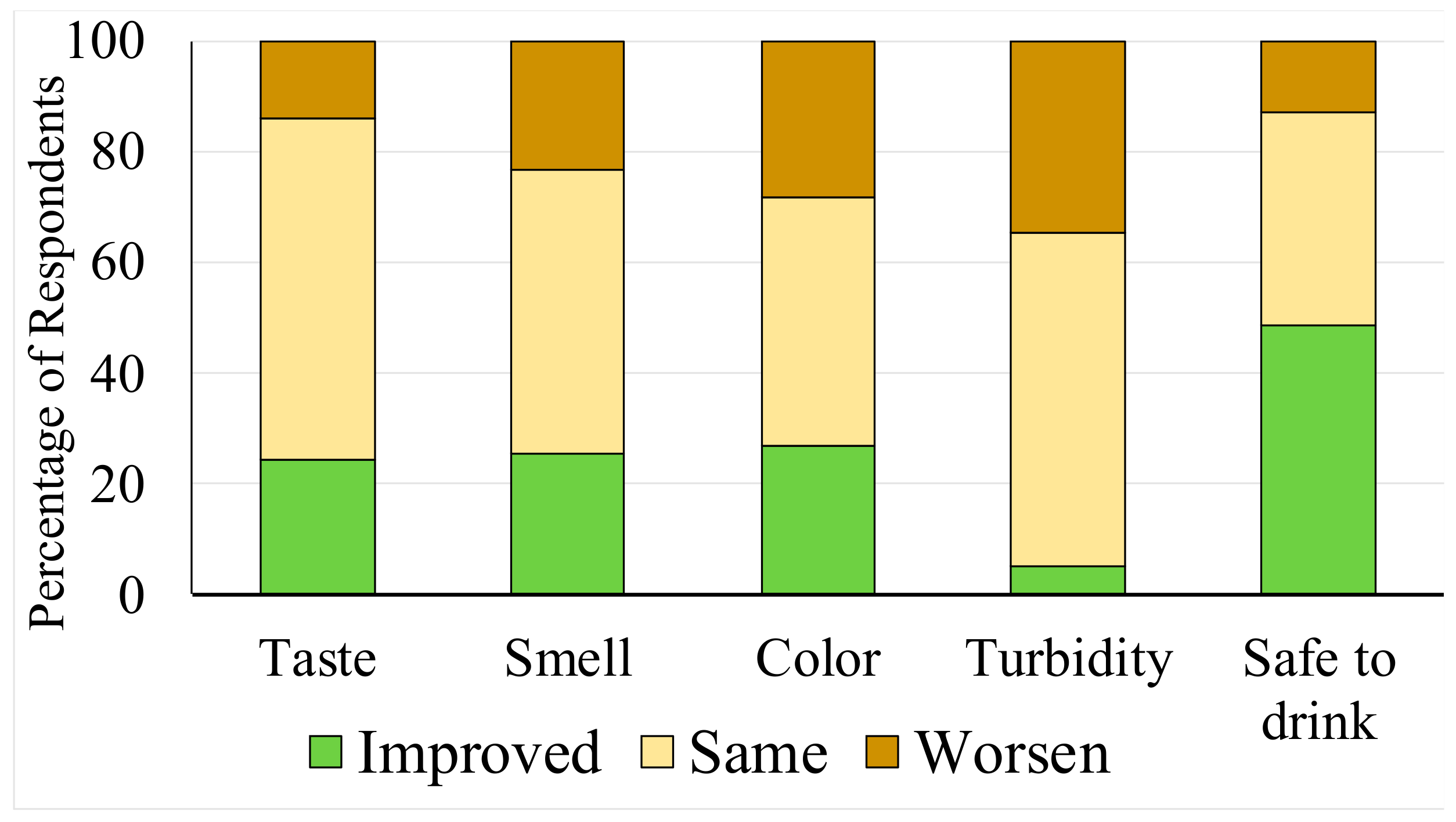
- Relative quality perception of LCD water: Change in as quality perception of the LCD water was compared with the previous drinking source and the social-club water by the following rankings: better, same, and worse.
2.6. Statistical Analysis
2.7. Ethical Consideration
3. Results
3.1. Quality of Source Water and LCD-Treated Water
3.2. Sociodemographic Characteristics of Respondents
3.3. Drinking Water Use Practices in the Pre-Intervention and Effects of Socioeconomic Parameters
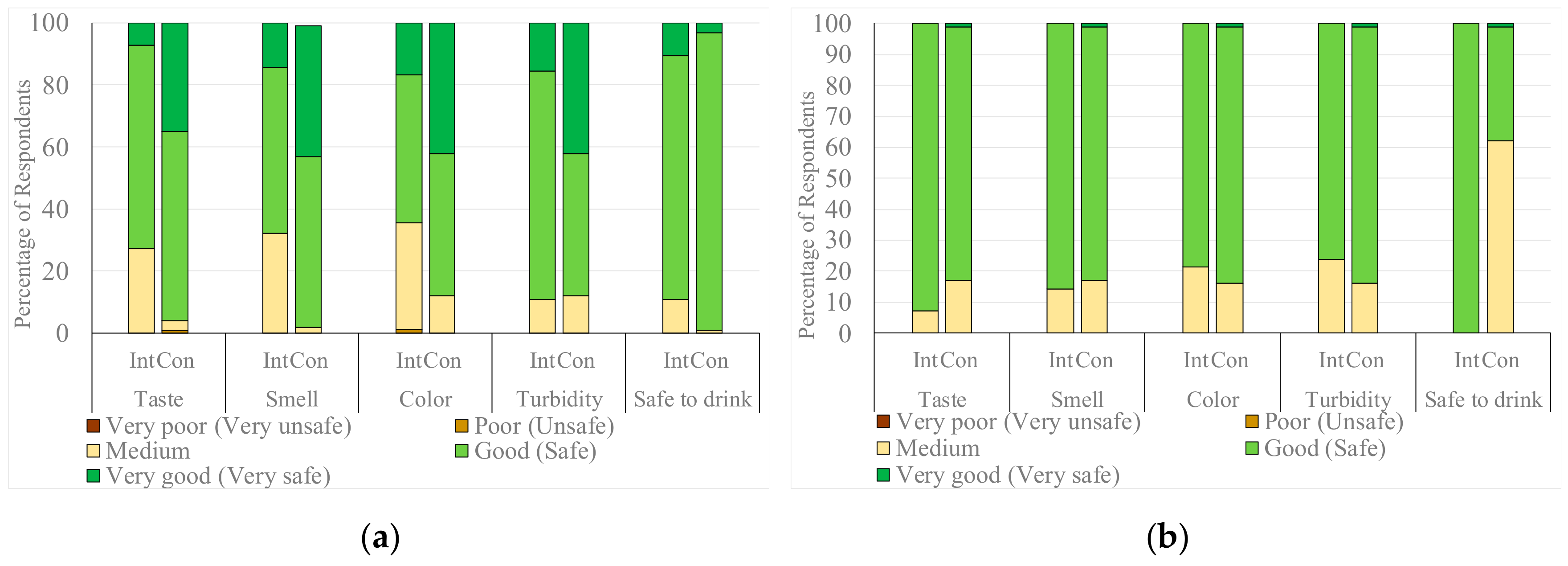
3.4. Quality Perceptions of Main Source of Drinking Water, WIS and QoL in the Pre-Intervention Period
3.5. Changes in Drinking Water Sources and Quality Perceptions of the Main Source of Drinking Water in the Post-Intervention Period
3.6. Statistical Evaluation of the Impact of LCD-Treated Water Supply
3.7. Relative Quality Perception of LCD Water with Previous Main Sources and Social-Club Water
4. Discussion
4.1. Water Quality Perception
4.2. In-House Water Treatment Practice and Cost
4.3. WIS and QoL Improvement
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wheater, H.S. Water Security: Science and management challenges. Proc. Int. Assoc. Hydrol. Sci. 2015, 366, 23–30. [Google Scholar] [CrossRef]
- The World Bank Water Overview. Available online: http://www.worldbank.org/en/topic/water/overview (accessed on 28 December 2017).
- Mekonnen, M.M.; Hoekstra, A.Y. Sustainability: Four billion people facing severe water scarcity. Sci. Adv. 2016, 2. [Google Scholar] [CrossRef] [PubMed]
- WWAP (United Nations World Water Assessment Programme). Water for a Sustainable World; United Nations Educational Scientific and Cultural Organization: Paris, France, 2015; ISBN 9789231000713. [Google Scholar]
- Surie, M.D. South Asia’ s Water Crisis: A Problem of Scarcity Amid Abundance. Available online: https://asiafoundation.org/2015/03/25/south-asias-water-crisis-a-problem-of-scarcity-amid-abundance/ (accessed on 12 March 2018).
- eSchooltoday Effects of Water Scarcity. Available online: http://www.eschooltoday.com/global-water-scarcity/effects-of-water-shortage.html (accessed on 7 April 2019).
- Rinkesh What Is Water Scarcity? Available online: https://www.conserve-energy-future.com/causes-effects-solutions-of-water-scarcity.php (accessed on 20 December 2018).
- Raditloaneng, W.N. Socio-Economic Factors in Rural Water Scarcity: A Case Study of Molepolole Village in Botswana. Am. J. Hum. Ecol. 2012, 1, 95–101. [Google Scholar]
- WHO Drinking Water-Fact Sheet. Available online: http://www.who.int/mediacentre/factsheets/fs391/en/ (accessed on 29 December 2017).
- Government of Nepal. Nepal Population and Housing Census 2011; Central Bureau of Statistics (CBS): Kathmandu, Nepal, 2012; Volume 01.
- Raina, A. Inequities in Household Water Consumption in Kathmandu, Nepal. Available online: http://www.globalwaterforum.org/2017/12/04/inequities-in-household-water-consumption-in-kathmandu-nepal/ (accessed on 3 September 2018).
- Chapagain, D.P. Urban Water Supply Sector Reform in Kathmandu Valley. J. Inst. Eng. 2012, 9, 130–141. [Google Scholar] [CrossRef]
- Thapa, B.R.; Ishidaira, H.; Pandey, V.P.; Bhandari, T.M.; Shakya, N.M. Evaluation of Water Security in Kathmandu Valley before and after Water Transfer from another Basin. Water 2018, 10, 224. [Google Scholar] [CrossRef]
- Aihara, Y.; Shrestha, S.; Kazama, F.; Nishida, K. Validation of household water insecurity scale in urban Nepal. Water Policy 2015, wp2015116. [Google Scholar] [CrossRef]
- ICIMOD. Kathmandu Valley Environment Outlook; ICIMOD: Kathmandu, Nepal, 2007. [Google Scholar]
- Shrestha, S.; Yoko, A.; Kondo, N.; Rajbhandari, S.; Bhattarai, A.P.; Bista, N.; Kazama, F.; Nishida, K.; Timilsina, H.P.; Shindo, J. Household Water Use in the Kathmandu Valley: A Dry Season Survey; ICRE WASH-MIA Report, ICRE; University of Yamanashi: Kofu, Japan, 2016. [Google Scholar]
- UN Water. Coping with Water Scarcity: A Strategic Issue and Priority for System-Wide Action; UN Water: Geneva, Switzerland, 2006. [Google Scholar]
- Meier, W.L.J. Climate, Climatic Change, and Water Supply; The National Academies Press: Washington, DC, USA, 1977; ISBN 978-0-309-02625-3. [Google Scholar]
- Asian Deveopment Bank. Tapping The Unreached: Nepal Small Towns Water Supply and Sanitation Sector Projects: A Sustainable Model of Service Delivery; ADB: Mandaluyong, Philippines, 2017. [Google Scholar]
- Aihara, Y.; Shrestha, S.; Sharma, J. Household water insecurity, depression and quality of life among postnatal women living in urban Nepal. J. Water Health 2016. [Google Scholar] [CrossRef]
- Shrestha, K.B.; Thapa, B.R.; Aihara, Y.; Shrestha, S.; Bhattarai, A.P.; Bista, N.; Kazama, F.; Shindo, J. Hidden Cost of Drinking Water Treatment and Its Relation with Socioeconomic Status in Nepalese Urban Context. Water 2018, 10, 607. [Google Scholar] [CrossRef]
- Osei-Asare, Y. Household Water Coping Behaviour and Costs in the Volta Basin of Ghana. In Proceedings of the Inaugural Symposium of the African Association of Agricultural Economists, Nairobi, Kenya, 6–8 December 2004; pp. 1–19. [Google Scholar]
- Koju, N.K.; Prasai, T.; Shrestha, S.M.; Raut, P. Drinking Water Quality of Kathmandu Valley. Nepal J. Sci. Technol. 2014, 15, 115–120. [Google Scholar] [CrossRef]
- Shrestha, S.; Malla, S.S.; Aihara, Y.; Kondo, N.; Nishida, K. Water Quality at Supply Source and Point of Use in the Kathmandu Valley. J. Water Environ. Technol. 2013, 11, 331–340. [Google Scholar] [CrossRef] [Green Version]
- Ghimire, G.; Adhikari, B.; Pradhan, M. Bacteriological Analysis of Water of Kathmandu Valley. Med. J. Shree Birendra Hosp. 2013, 12, 19–22. [Google Scholar] [CrossRef]
- Bhandari, P.; Khanal, S.; Shakya, R.; Joshi, D.R. Microbial Quality of Jar Water sold in Kathmandu Valley. J. Food Sci. Technol. 2009, 5, 150–152. [Google Scholar]
- Subedi, M.; Aryal, M. Public perception about drinking jar water and its bacteriological analysis. Nepal Med. Coll. J. 2010, 12, 110–114. [Google Scholar]
- Chapagain, S.K.; Shrestha, S.; Nakamura, T.; Pandey, V.P.; Kazama, F. Arsenic occurrence in groundwater of Kathmandu Valley, Nepal. Desalin. Water Treat. 2009, 4, 248–254. [Google Scholar] [CrossRef]
- Pant, B.R. Groundwater quality in the Kathmandu valley of Nepal. Environ. Monit. Assess. 2011, 178, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Warner, N.R.; Levy, J.; Harpp, K.; Farruggia, F. Drinking water quality in Nepal’s Kathmandu Valley: A survey and assessment of selected controlling site characteristics. Hydrogeol. J. 2008, 16, 321–334. [Google Scholar] [CrossRef]
- Khatiwada, N.R.; Takizawa, S.; Tran, T.V.N.; Inoue, M. Groundwater contamination assessment for sustainable water supply in Kathmandu Valley, Nepal. Water Sci. Technol. 2002, 46, 147–154. [Google Scholar] [CrossRef]
- Pandey, V.P.; Shrestha, S.; Kazama, F. Groundwater in the Kathmandu Valley: Development dynamics, consequences and prospects for sustainable management. Eur. Water 2012, 37, 3–14. [Google Scholar]
- Pattanayak, S.K.; Yang, J.-C.C.; Whittington, D.; Bal Kumar, K.C. Coping with unreliable public water supplies: Averting expenditures by households in Kathmandu, Nepal. Water Resour. Res. 2005, 41, 1–11. [Google Scholar] [CrossRef]
- Clasen, T.F.; Alexander, K.T.; Sinclair, D.; Boisson, S.; Peletz, R.; Chang, H.H.; Majorin, F.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Clasen, T.; Schmidt, W.-P.; Rabie, T.; Roberts, I.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea: Systematic review and meta-analysis. BMJ 2007, 334, 782. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.L.; Kahawita, T.M.; Cairncross, S.; Ensink, J.H.J. The Impact of Water, Sanitation and Hygiene Interventions to Control Cholera: A Systematic Review. PLoS ONE 2015, 10, e0135676. [Google Scholar] [CrossRef] [PubMed]
- Gundry, S.; Wright, J.; Conroy, R. A systematic review of the health outcomes related to household water quality in developing countries. J. Water Health 2004, 2, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevenson, E.G.J.J.; Ambelu, A.; Caruso, B.A.; Tesfaye, Y.; Freeman, M.C.; Lindstrom, D. Community Water Improvement, Household Water Insecurity, and Women’s Psychological Distress: An Intervention and Control Study in Ethiopia. PLoS ONE 2016, 11, e0153432. [Google Scholar] [CrossRef] [PubMed]
- WSUP AND SHARE. Evaluating the Health Impact of Urban WASH Programmes: An Affordable Approach for Enhancing Effectiveness; WSUP: London, UK, 2011; pp. 1–32.
- Khanitchaidecha, W.; Shakya, M.; Nakano, Y.; Tanaka, Y.; Kazama, F. Development of an attached growth reactor for NH 4-N removal at a drinking water supply system in Kathmandu Valley, Nepal. J. Environ. Sci. Health Part A Toxic/Hazard. Subst. Environ. Eng. 2012, 47, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Physical Planning and Works Government of Nepal. National Drinking Water Quality Standards, Implementation Directives for National Drinking Water Quality Standards, 2005; Ministry of Physical Planning and Works Government of Nepal: Kathmandu, Nepal, 2005.
- Columbia University Population Health Methods: Difference-in-Difference Estimation. Available online: https://www.mailman.columbia.edu/research/population-health-methods/difference-difference-estimation (accessed on 18 January 2019).
- Rutstein, S.O.; Johnson, K. The DHS Wealth Index, DHS Comparative Report 6; ORC Macro: Calverton, MD, USA, 2004. [Google Scholar]
- Francis, M.R.; Nagarajan, G.; Sarkar, R.; Mohan, V.R.; Kang, G.; Balraj, V. Perception of drinking water safety and factors influencing acceptance and sustainability of a water quality intervention in rural southern India. BMC Public Health 2015, 15, 1–9. [Google Scholar] [CrossRef]
- Rojas, L.F.R.; Megerle, A.; Araral, E. Perception of Water Quality and Health Risks in the Rural Area of Medellín. Am. J. Rural Dev. 2010, 12, 106–115. [Google Scholar] [CrossRef]
- De França Doria, M. Factors influencing public perception of drinking water quality. Water Policy 2010, 12, 1–19. [Google Scholar] [CrossRef]
- De França Doria, M.; Pidgeon, N.; Hunter, P.R. Perceptions of drinking water quality and risk and its effect on behaviour: A cross-national study. Sci. Total Environ. 2009, 407, 5455–5464. [Google Scholar] [CrossRef]
- Onjala, J.; Ndiritu, S.W.; Stage, J. Risk Perception, Choice of Drinking Water, and Water Treatment. J. Water Sanit. Hyg. Dev. 2014, 4, 268–280. [Google Scholar] [CrossRef]
- Lilje, J.; Kessely, H.; Mosler, H.-J. Factors determining water treatment behavior for the prevention of cholera in Chad. Am. J. Trop. Med. Hyg. 2015, 93, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, E.G.J.; Greene, L.E.; Maes, K.C.; Ambelu, A.; Tesfaye, Y.A.; Rheingans, R.; Hadley, C. Water insecurity in 3 dimensions: An anthropological perspective on water and women’s psychosocial distress in Ethiopia. Soc. Sci. Med. 2012, 75, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Katuwal, H.; Bohara, A.K. Coping with poor water supplies: Empirical evidence from Kathmandu, Nepal. J. Water Health 2011, 9, 143–158. [Google Scholar] [CrossRef] [PubMed]
- Wikipedia Quality of Life. Available online: https://en.wikipedia.org/wiki/Quality_of_life (accessed on 6 November 2018).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Socioeconomic Characteristics | Intervention (Chyasal) HH Number (%) 2 | Control (Kumbheshwor) HH Number (%) | p Value 3 | |
|---|---|---|---|---|
| Age group | Less than 40 years | 33 (39.3) | 50 (50.0) | 0.146 C |
| 40 years and older | 51(60.7) | 50 (50.0) | ||
| Ethnicity | Brahmin/Chhetri | 4 (4.8) | 3 (3.0) | 0.309 C |
| Newar | 78 (92.9) | 97 (97.0) | ||
| Janajati | 1 (1.2) | 0 (0.0) | ||
| Dalit | 1 (1.2) | 0 (0.0) | ||
| Education | Illiterate | 19 (22.6) | 16 (16.0) | 0.907 U |
| School level (1–10) | 33 (39.3) | 50 (50.0) | ||
| High School and above | 32 (38.1) | 34 (34.0) | ||
| Occupation | Unemployed | 37 (44.0) | 38 (38.0) | 0.544 C |
| Daily employed | 16 (19.0) | 25 (25.0) | ||
| Business | 14 (16.7) | 23 (23.0) | ||
| Service | 17 (20.2) | 14 (14.0) | ||
| Economic quintile | Poorest | 18 (21.4) | 17 (17.0) | 0.200 U |
| Poorer | 9 (10.7) | 29 (29.0) | ||
| Medium | 22 (26.2) | 15 (15.0) | ||
| Richer | 12 (14.3) | 26 (26.0) | ||
| Richest | 23 (27.4) | 13 (13.0) | ||
| Family size | <5 members | 49 (58.3) | 49 (49.0) | 0.206 C |
| ≥5 members | 35 (41.7) | 51 (51.0) | ||
| Household ownership | Own | 77 (91.7) | 97 (97.0) | 0.110 C |
| Rented | 7 (8.3) | 3 (3.0) | ||
| SN | Water Use | INT | CON | β | Sig. | Age | Edu | Occ | WQ | Fsize | HH Own |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | PW used for drinking | 60.7 | 5.0 | 3.691 | 0.000 | ||||||
| 2 | JW used for drinking | 16.7 | 61.0 | −2.244 | 0.000 | ||||||
| 3 | SCW used for drinking | 41.7 | 16.0 | 1.277 | 0.002 | * | |||||
| 4 | GW used for drinking | 9.5 | 22.0 | −1.375 | 0.009 | * | |||||
| 5 | TV water used for drinking | 22.6 | 4.0 | 2.342 | 0.000 | * | |||||
| 6 | Treat drinking water | 96.0 | 85.0 | 1.806 | 0.017 | * | |||||
| 7 | Ceramic filter use | 75.0 | 67.0 | 0.421 | 0.261 | ||||||
| 8 | Boiling | 71.4 | 55.0 | 0.919 | 0.015 | ** | * | ||||
| 9 | Euro-guard use | 7.1 | 2.0 | 0.737 | 0.447 |
| SN | Water Use | INT | CON | β | Sig. | Age | Edu | Occ | WQ | Fsize | HH Own |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Water Insecurity Score (WIS) | 2.04 | 1.65 | 0.411 | 0.000 | ||||||
| 2 | Quality of life | 3.31 | 3.80 | −0.509 | 0.000 | ** | ** | ** |
| SN | Impact Variables | Time Effect (βt) | Place Effect (βp) | (DiD = βt.p) | Socioeconomic Parameters 2 | Time Effect at Intervention Site (βt1) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted (β) Coff | p Value | Adjusted (β) Coff | p Value | Adjusted (β) Coff | p Value | Age | Edu | Occ | WQ | Adjusted (β) Coff | p Value | ||
| 1 | DW taste perception | −1.68 | 0.004 | −2.16 | 0.000 | 3.18 | 0.000 | 1.49 | 0.003 | ||||
| 2 | DW smell perception | −2.43 | 0.002 | −3.19 | 0.000 | 3.39 | 0.000 | * | 0.96 | 0.020 | |||
| 3 | DW color perception | −0.35 | 0.393 | −1.43 | 0.000 | 0.94 | 0.088 | 0.59 | 0.106 | ||||
| 4 | DW turbidity perception | −0.50 | 0.222 | 0.38 | 0.467 | −0.78 | 0.218 | −1.27 | 0.008 | ||||
| 5 | Safe to drink 3 | −5.41 | 0.000 | −2.40 | 0.027 | -- | -- | * | 20.38 | 0.998 | |||
| 6 | DW Treatment | 0.13 | 0.003 | 0.11 | 0.020 | −0.44 | 0.000 | −0.31 | 0.000 | ||||
- Binary logistic regression was applied.
- *: significant at 5% level.
- β coefficient of intervention site and DiD cannot be calculated because 100% of households perceived the water was safe to drink in the post-intervention.
| SN | Impact Variables | Time Effect (βt) | Place Effect (βp) | (DiD= βt.p) | Socioeconomic Parameters 2 | Time Effect at Intervention Site (βt1) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted (β) Coff | p Value | Adjusted (β) Coff | p Value | Adjusted (β) Coff | p Value | Age | Edu | Occ | WQ | Adjusted (β) Coff | p Value | ||
| 1 | Water Insecurity Score | 0.47 | 0.000 | 0.39 | 0.000 | 0.61 | 0.000 | * | −0.14 | 0.071 | |||
| 2 | Quality of Life Score | 0.14 | 0.071 | −0.49 | 0.000 | 0.65 | 0.000 | ** | ** | ** | 0.22 | 0.000 | |
- Linear regression was applied
| SN | Impact Variables | Intervention Site | Control Site | ||||
|---|---|---|---|---|---|---|---|
| HH no | Pre-int | Post-int | HH no | Pre-int | Post-int | ||
| 1 | DW taste perception | 78 | 74% | 92% | 100 | 96% | 83% |
| 2 | DW smell perception | 78 | 69% | 85% | 100 | 98% | 83% |
| 3 | DW color perception | 78 | 65% | 77% | 100 | 88% | 84% |
| 4 | DW turbidity perception | 78 | 91% | 74% | 100 | 88% | 82% |
| 5 | Safe to drink | 78 | 90% | 100% | 100 | 99% | 38% |
| 6 | DW Treatment | 84 | 96% | 65% | 100 | 85% | 98% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shrestha, K.B.; Kamei, T.; Shrestha, S.; Aihara, Y.; Bhattarai, A.P.; Bista, N.; Thapa, B.R.; Kazama, F.; Shindo, J. Socioeconomic Impacts of LCD-Treated Drinking Water Distribution in an Urban Community of the Kathmandu Valley, Nepal. Water 2019, 11, 1323. https://doi.org/10.3390/w11071323
Shrestha KB, Kamei T, Shrestha S, Aihara Y, Bhattarai AP, Bista N, Thapa BR, Kazama F, Shindo J. Socioeconomic Impacts of LCD-Treated Drinking Water Distribution in an Urban Community of the Kathmandu Valley, Nepal. Water. 2019; 11(7):1323. https://doi.org/10.3390/w11071323
Chicago/Turabian StyleShrestha, Khadga Bahadur, Tatsuru Kamei, Sadhana Shrestha, Yoko Aihara, Arun Prasad Bhattarai, Niranjan Bista, Bhesh Raj Thapa, Futaba Kazama, and Junko Shindo. 2019. "Socioeconomic Impacts of LCD-Treated Drinking Water Distribution in an Urban Community of the Kathmandu Valley, Nepal" Water 11, no. 7: 1323. https://doi.org/10.3390/w11071323