
Effects of Oral Cannabidiol on Health and Fitness in Healthy Adults: An 8-Week Randomized Trial
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Overview
2.2. Subjects
2.3. Procedures
2.3.1. Body Size and Composition Assessments
2.3.2. Aerobic Fitness Assessment
2.3.3. Anaerobic Fitness Assessment
2.3.4. Muscular Strength Assessment
2.3.5. Physical Activity Assessment
2.3.6. Measures of Mental Health and Wellbeing
2.3.7. Blood Collection and CRP
2.4. Statistical Analyses
3. Results
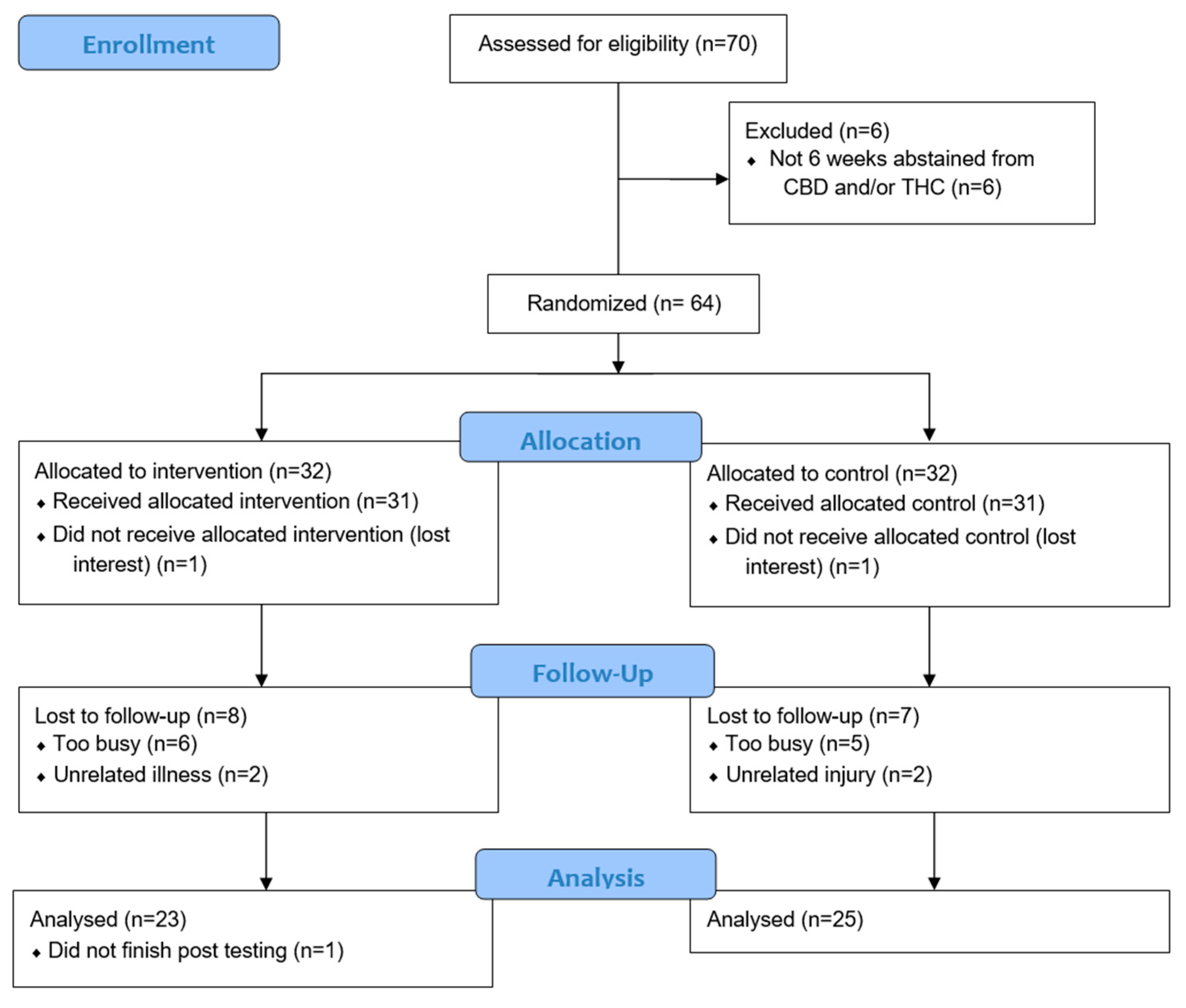
3.1. Subjects
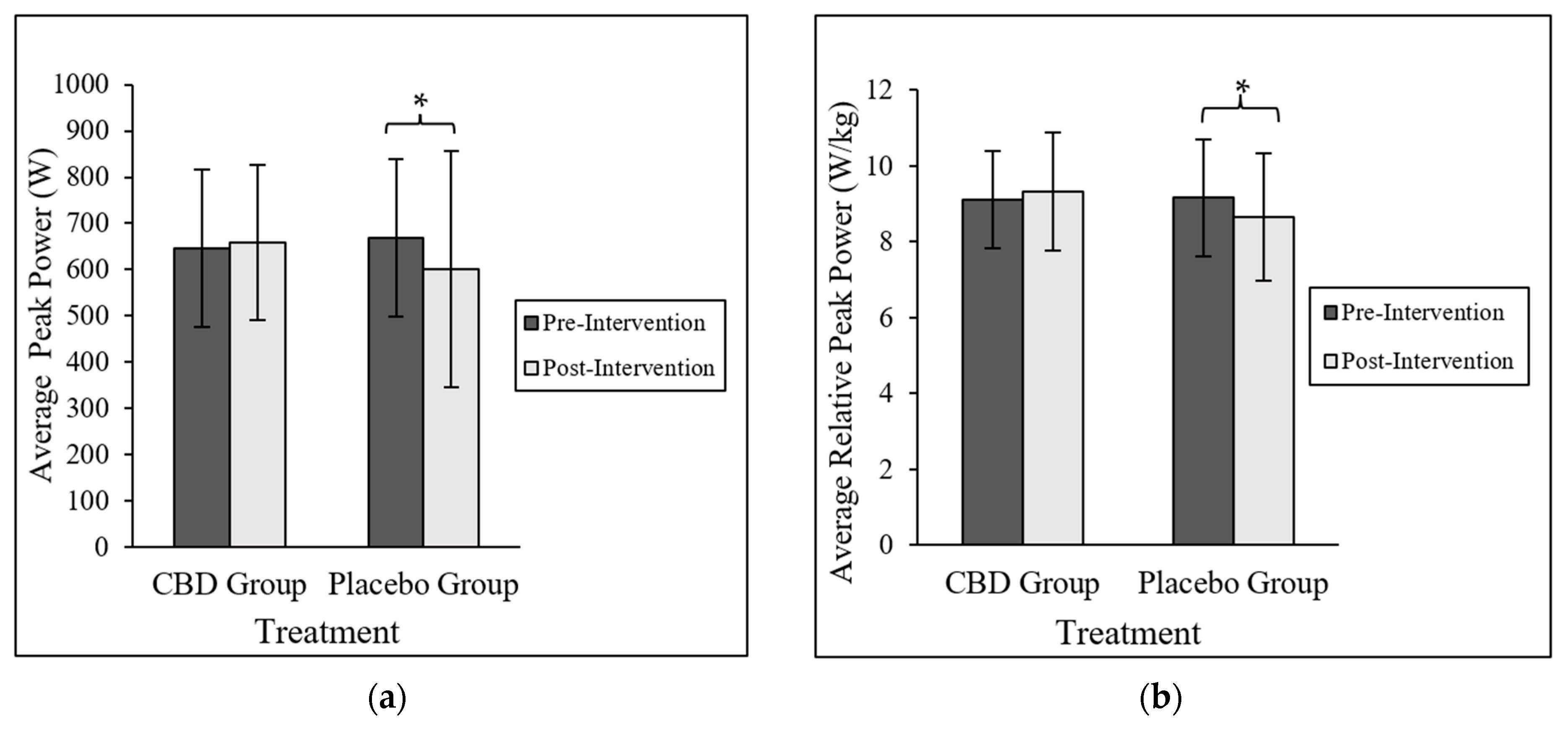
3.2. Health-Related Fitness
3.3. Physical Activity Measures
3.4. Measures of Mental Health and Wellbeing
3.5. Resting Concentrations of CRP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gáll, Z.; Farkas, S.; Albert, A.; Ferencz, E.; Vancea, S.; Urkon, M.; Kolcsár, M. Effects of Chronic Cannabidiol Treatment in the Rat Chronic Unpredictable Mild Stress Model of Depression. Biomolecules 2020, 10, 801. [Google Scholar] [CrossRef] [PubMed]
- Sales, A.J.; Guimarães, F.S.; Joca, S.R. CBD modulates DNA methylation in the prefrontal cortex and hippocampus of mice exposed to forced swim. Behav. Brain Res. 2020, 388, 112627. [Google Scholar] [CrossRef] [PubMed]
- Maroon, J.; Bost, J. Review of the neurological benefits of phytocannabinoids. Surg. Neurol. Int. 2018, 9, 91. [Google Scholar] [CrossRef]
- Solowij, N.; Broyd, S.J.; Beale, C.; Prick, J.-A.; Greenwood, L.-M.; van Hell, H.; Suo, C.; Galettis, P.; Pai, N.; Fu, S.; et al. Therapeutic Effects of Prolonged Cannabidiol Treatment on Psychological Symptoms and Cognitive Function in Regular Cannabis Users: A Pragmatic Open-Label Clinical Trial. Cannabis Cannabinoid Res. 2018, 3, 21–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Premoli, M.; Aria, F.; Bonini, S.A.; Maccarinelli, G.; Gianoncelli, A.; Della Pina, S.; Tambaro, S.; Memo, M.; Mastinu, A. Cannabidiol: Recent advances and new insights for neuropsychiatric disorders treatment. Life Sci. 2019, 224, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Peres, F.F.; Lima, A.C.; Hallak, J.E.C.; Crippa, J.A.; Silva, R.; Abilio, V. Cannabidiol as a Promising Strategy to Treat and Prevent Movement Disorders? Front. Pharmacol. 2018, 9, 482. [Google Scholar] [CrossRef] [Green Version]
- Pertwee, R.G. The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: Δ9-tetrahydrocannabinol, cannabidiol and Δ9-tetrahydrocannabivarin. Br. J. Pharmacol. 2008, 153, 199–215. [Google Scholar] [CrossRef] [Green Version]
- Jîtcă, G.; Ősz, B.E.; Vari, C.E.; Rusz, C.-M.; Tero-Vescan, A.; Pușcaș, A. Cannabidiol: Bridge between Antioxidant Effect, Cellular Protection, and Cognitive and Physical Performance. Antioxidants 2023, 12, 485. [Google Scholar] [CrossRef]
- Lazarini-Lopes, W.; Silva, R.A.D.V.-D.; da Silva-Júnior, R.M.; Leite, J.P.; Garcia-Cairasco, N. The anticonvulsant effects of cannabidiol in experimental models of epileptic seizures: From behavior and mechanisms to clinical insights. Neurosci. Biobehav. Rev. 2020, 111, 166–182. [Google Scholar] [CrossRef]
- Atalay, S.; Jarocka-Karpowicz, I.; Skrzydlewska, E. Antioxidative and Anti-Inflammatory Properties of Cannabidiol. Antioxidants 2019, 9, 21. [Google Scholar] [CrossRef] [Green Version]
- Privitera, M.; Bhathal, H.; Wong, M.; Cross, J.H.; Wirrell, E.; Marsh, E.D.; Mazurkiewicz-Beldzinska, M.; Villanueva, V.; Checketts, D.; Knappertz, V.; et al. Time to onset of cannabidiol (CBD) treatment effect in Lennox–Gastaut syndrome: Analysis from two randomized controlled trials. Epilepsia 2021, 62, 1130–1140. [Google Scholar] [CrossRef] [PubMed]
- Reddy, D.S.; Mbilinyi, R.H.; Ramakrishnan, S. Efficacy of the FDA-approved cannabidiol on the development and persistence of temporal lobe epilepsy and complex focal onset seizures. Exp. Neurol. 2023, 359, 114240. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yan, X.; Wang, Z.; Ma, M.; Zhang, B.; Jia, Z. Comparison of the Users’ Attitudes Toward Cannabidiol on Social Media Platforms: Topic Modeling Study. JPHS 2023, 9, e34132. [Google Scholar] [CrossRef] [PubMed]
- Kasper, A.M.; Sparks, S.A.; Hooks, M.; Skeer, M.; Webb, B.; Nia, H.; Morton, J.P.; Close, G.L. High Prevalence of Cannabidiol Use Within Male Professional Rugby Union and League Players: A Quest for Pain Relief and Enhanced Recovery. Int. J. Sport Nutr. Exerc. Metab. 2020, 30, 315–322. [Google Scholar] [CrossRef]
- Moltke, J.; Hindocha, C. Reasons for cannabidiol use: A cross-sectional study of CBD users, focusing on self-perceived stress, anxiety, and sleep problems. J. Cannabis Res. 2021, 3, 5. [Google Scholar] [CrossRef]
- Crossland, B.W.; Rigby, B.R.; Duplanty, A.A.; King, G.A.; Juma, S.; Levine, N.A.; Clark, C.E.; Ramirez, K.P.; Varone, N.L. Acute Supplementation with Cannabidiol Does Not Attenuate Inflammation or Improve Measures of Performance following Strenuous Exercise. Healthcare 2022, 10, 1133. [Google Scholar] [CrossRef]
- Isenmann, E.; Veit, S.; Starke, L.; Flenker, U.; Diel, P. Effects of Cannabidiol Supplementation on Skeletal Muscle Regeneration after Intensive Resistance Training. Nutrients 2021, 13, 3028. [Google Scholar] [CrossRef]
- Cochrane-Snyman, K.C.; Cruz, C.; Morales, J.; Coles, M. The Effects of Cannabidiol Oil on Noninvasive Measures of Muscle Damage in Men. Med. Sci. Sports Exerc. 2021, 53, 1460–1472. [Google Scholar] [CrossRef]
- Stone, W.J.; Tolusso, D.V.; Pancheco, G.; Brgoch, S.; Nguyen, V.T. A Pilot Study on Cannabidiol (CBD) and Eccentric Exercise: Impact on Inflammation, Performance, and Pain. Int. J. Exerc. Sci. 2023, 16, 109–117. [Google Scholar]
- Erukainure, O.L.; Matsabisa, M.G.; Salau, V.F.; Olofinsan, K.A.; Oyedemi, S.O.; Chukwuma, C.I.; Nde, A.L.; Islam, M.S. Cannabidiol improves glucose utilization and modulates glucose-induced dysmetabolic activities in isolated rats’ peripheral adipose tissues. Biomed. Pharmacother. 2022, 149, 112863. [Google Scholar] [CrossRef]
- Parray, H.A.; Yun, J.W. Cannabidiol promotes browning in 3T3-L1 adipocytes. Mol. Cell. Biochem. 2016, 416, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Abbotts, K.S.S.; Ewell, T.R.; Butterklee, H.M.; Bomar, M.C.; Akagi, N.; Dooley, G.P.; Bell, C. Cannabidiol and Cannabidiol Metabolites: Pharmacokinetics, Interaction with Food, and Influence on Liver Function. Nutrients 2022, 14, 2152. [Google Scholar] [CrossRef] [PubMed]
- Sahinovic, A.; Irwin, C.; Doohan, P.T.; Kevin, R.C.; Cox, A.J.; Lau, N.S.; Ben Desbrow, B.; Johnson, N.A.; Sabag, A.; Hislop, M.; et al. Effects of Cannabidiol on Exercise Physiology and Bioenergetics: A Randomised Controlled Pilot Trial. Sports Med. Open 2022, 8, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Morris, E.M.; Kitts-Morgan, S.E.; Spangler, D.M.; Gebert, J.; Vanzant, E.S.; McLeod, K.R.; Harmon, D.L. Feeding Cannabidiol (CBD)-Containing Treats Did Not Affect Canine Daily Voluntary Activity. Front. Vet. Sci. 2021, 8, 645667. [Google Scholar] [CrossRef]
- McGuire, P.; Robson, P.; Cubala, W.J.; Vasile, D.; Morrison, P.D.; Barron, R.; Taylor, A.; Wright, S. Cannabidiol (CBD) as an Adjunctive Therapy in Schizophrenia: A Multicenter Randomized Controlled Trial. Am. J. Psychiatry 2018, 175, 225–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloomfield, M.; Green, S.F.; Hindocha, C.; Yamamori, Y.; Yim, J.L.L.; Jones, A.P.M.; Walker, H.R.; Tokarczuk, P.; Statton, B.; Howes, O.D.; et al. The effects of acute cannabidiol on cerebral blood flow and its relationship to memory: An arterial spin labelling magnetic resonance imaging study. J. Psychopharmacol. 2020, 34, 981–989. [Google Scholar] [CrossRef]
- Corroon, J.; Phillips, J.A. A Cross-Sectional Study of Cannabidiol Users. Cannabis Cannabinoid Res. 2018, 3, 152–161. [Google Scholar] [CrossRef] [Green Version]
- Morissette, F.; Mongeau-Pérusse, V.; Rizkallah, E.; Thébault, P.; Lepage, S.; Brissette, S.; Bruneau, J.; Dubreucq, S.; Stip, E.; Cailhier, J.-F.; et al. Exploring cannabidiol effects on inflammatory markers in individuals with cocaine use disorder: A randomized controlled trial. Neuropsychopharmacology 2021, 46, 2101–2111. [Google Scholar] [CrossRef]
- Marini, S.; Huber, A.; Cash, M.N.; Salemi, M.; Cook, R.L.; Borsa, P.; Mavian, C.N. Oral CBD treatment is associated to an anti-inflammatory gene expression signature in myeloid cells of people living with HIV. medRxiv 2023. [Google Scholar] [CrossRef]
- Jadoon, K.A.; Ratcliffe, S.H.; Barrett, D.A.; Thomas, E.L.; Stott, C.; Bell, J.D.; O’sullivan, S.E.; Tan, G.D. Efficacy and Safety of Cannabidiol and Tetrahydrocannabivarin on Glycemic and Lipid Parameters in Patients with Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled, Parallel Group Pilot Study. Diabetes Care 2016, 39, 1777–1786. [Google Scholar] [CrossRef] [Green Version]
- Pescatello, L.; Arena, R.; Riebe, D.; Thompson, P. Health-Related Physical Fitness Testing and Interpretation, in ACSM’s Guidelines for Exercise Testing and Prescription 2014; Wolters Kluwer/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014; pp. 73–76. [Google Scholar]
- Bar-Or, O. The Wingate anaerobic test. An update on methodology, reliability and validity. Sports Med. 1987, 4, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Baechle, T.R.; Earle, R.W. Essentials of Strength Training and Conditioning, 3rd ed; Human Kinetics: Champaign, IL, USA, 2008; p. 395. [Google Scholar]
- Valentine, T.R.; Weiss, D.M.; Jones, J.A.; Andersen, B.L. Construct validity of PROMIS® Cognitive Function in cancer patients and noncancer controls. Health Psychol. 2019, 38, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Ryff, C.D.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Pers. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Stewart, L.K.; Flynn, M.G.; Campbell, W.W.; Craig, B.A.; Robinson, J.P.; Timmerman, K.L.; Mcfarlin, B.K.; Coen, P.M.; Talbert, E. The Influence of Exercise Training on Inflammatory Cytokines and C-Reactive Protein. Med. Sci. Sports Exerc. 2007, 39, 1714–1719. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; pp. 17–25. [Google Scholar]
- Zhang, J.; Luo, Z.; Zhang, Z.; Zhao, M.; Tong, C.; Cong, P.; Mao, S.; Zhao, Y.; Hou, M.; Piao, Y.; et al. Protective effect and mechanism of cannabidiol on myocardial injury in exhaustive exercise training mice. Chem. Biol. Interact. 2022, 365, 110079. [Google Scholar] [CrossRef]
- Hampson, A.J.; Grimaldi, M.; Axelrod, J.; Wink, D. Cannabidiol and (−)Δ 9 -tetrahydrocannabinol are neuroprotective antioxidants. Proc. Natl. Acad. Sci. USA 1998, 95, 8268–8273. [Google Scholar] [CrossRef] [Green Version]
- Borges, R.; da Silva, A. Cannabidiol as an Antioxidant. Handbook of Cannabis and Related Pathologies; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Fernández-Ruiz, J.; Garcia, C.; Sagredo, O.; Ruiz, M.G.; DE Lago, E. The endocannabinoid system as a target for the treatment of neuronal damage. Expert Opin. Ther. Targets 2010, 14, 387–404. [Google Scholar] [CrossRef]
- Li, L.; Xuan, Y.; Zhu, B.; Wang, X.; Tian, X.; Zhao, L.; Wang, Y.; Jiang, X.; Wen, N. Protective Effects of Cannabidiol on Chemotherapy-Induced Oral Mucositis via the Nrf2/Keap1/ARE Signaling Pathways. Oxidative Med. Cell. Longev. 2022, 2022, 4619760. [Google Scholar] [CrossRef]
- Vomund, S.; Schäfer, A.; Parnham, M.J.; Brüne, B.; Von Knethen, A. Nrf2, the Master Regulator of Anti-Oxidative Responses. Int. J. Mol. Sci. 2017, 18, 2772. [Google Scholar] [CrossRef] [Green Version]
- Bielawiec, P.; Dziemitko, S.; Konstantynowicz-Nowicka, K.; Chabowski, A.; Dzięcioł, J.; Harasim-Symbor, E. Cannabidiol improves muscular lipid profile by affecting the expression of fatty acid transporters and inhibiting de novo lipogenesis. Sci. Rep. 2023, 13, 3694. [Google Scholar] [CrossRef]
- Lopez, H.L.; Cesareo, K.R.; Raub, B.; Kedia, A.W.; Sandrock, J.E.; Kerksick, C.M.; Ziegenfuss, T.N. Effects of Hemp Extract on Markers of Wellness, Stress Resilience, Recovery and Clinical Biomarkers of Safety in Overweight, But Otherwise Healthy Subjects. J. Diet. Suppl. 2020, 17, 561–586. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.d.S.; Jantsch, J.; Fraga, G.d.F.; Dias, V.S.; Eller, S.; De Oliveira, T.F.; Giovenardi, M.; Guedes, R.P. Cannabidiol treatment improves metabolic profile and decreases hypothalamic inflammation caused by maternal obesity. Front. Nutr. 2023, 10, 385. [Google Scholar] [CrossRef] [PubMed]
- Le Strat, Y.; Le Foll, B. Obesity and Cannabis Use: Results From 2 Representative National Surveys. Am. J. Epidemiol. 2011, 174, 929–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedorova, E.V.; Wong, C.F.; Ataiants, J.; Iverson, E.; Conn, B.M.; Lankenau, S.E. Cannabidiol (CBD) and other drug use among young adults who use cannabis in Los Angeles. Drug Alcohol Depend. 2021, 221, 108648. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. Clinical application of C-reactive protein for cardiovascular disease detection and prevention. Circulation 2003, 107, 363–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brady, C.M.; Dasgupta, R.; Dalton, C.; Wiseman, O.J.; Berkley, K.J.; Fowler, C.J. An open-label pilot study of cannabis-based extracts for bladder dysfunction in advanced multiple sclerosis. Mult. Scler. J. 2004, 10, 425–433. [Google Scholar] [CrossRef]
- Huestis, M.A.; Solimini, R.; Pichini, S.; Pacifici, R.; Carlier, J.; Busardò, F.P. Cannabidiol Adverse Effects and Toxicity. Curr. Neuropharmacol. 2019, 17, 974–989. [Google Scholar] [CrossRef]
- Cooper, Z.D.; Craft, R.M. Sex-Dependent Effects of Cannabis and Cannabinoids: A Translational Perspective. Neuropsychopharmacology 2017, 43, 34–51. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | CG | PG | Overall | p |
|---|---|---|---|---|
| Age (years) | 24.3 ± 4.5 | 26.5 ± 6.5 | 25.5 ± 5.7 | 0.165 |
| Height (cm) | 170.1 ± 9.7 | 171.2 ± 9.8 | 171 ± 10 | 0.700 |
| Body mass (kg) | 72.4 ± 15.5 | 73.3 ± 10.6 | 73.6 ± 13.7 | 0.884 |
| Resting heart rate (bpm) | 68 ± 7 | 66.2 ± 11.1 | 67 ± 9 | 0.366 |
| Resting systolic blood (mmHg) | 117 ± 8.2 | 118 ± 11.4 | 118 ± 10 | 0.955 |
| Resting diastolic blood (mmHg) | 74.5 ± 7.2 | 74.6 ± 7.3 | 75.1 ± 7 | 0.652 |
| Health-Related Fitness Variable | Pre-CG | Pre-PG | Post-CG | Post-PG |
|---|---|---|---|---|
| Lean body mass (kg) | 57 ± 12.4 | 56.8 ± 11.1 | 58.8 ± 12.5 | 57.8 ± 12.4 |
| Body fat percentage (%) | 20.9 ± 8.3 | 22.1 ± 9.1 | 20.9 ± 8.2 | 23.1 ± 9.1 |
| Relative VO2 peak (mL·min−1·kg−1) | 45 ± 8.2 | 43.0 ± 7.2 | 45.9 ± 8.2 | 42.8 ± 8 |
| Bench press 1RM (kg) | 66.1 ± 31 | 64.5 ± 33.7 | 67.4 ± 30 | 65.7 ± 34.8 |
| Back squat 1RM (kg) | 94.6 ± 29.1 | 88.7 ± 34.2 | 98 ± 28.6 | 93.3 ± 32.8 |
| Anaerobic Output Variable | Pre-CG | Pre-PG | Post-CG | Post-PG |
|---|---|---|---|---|
| Mean power (W) | 485 ± 127 | 476.7 ± 126.6 | 486.3 ± 126.6 | 467.2 ± 140.6 |
| Relative mean power (W/kg) | 6.6 ± 1 | 6.4 ± 1.2 | 6.6 ± 1 | 6.3 ± 1.3 |
| Anaerobic fatigue (%) | 57.1 ± 7.9 | 56 ± 6 | 58.9 ± 6.1 | 58.0 ± 9.1 |
| Survey | Pre-CG | Pre-PG | Post-CG | Post-PG |
|---|---|---|---|---|
| Cognitive Function T-Scores | 49 ± 6.6 | 48.4 ± 9.6 | 48.8 ± 6.8 | 47.8 ± 11.8 |
| Cognitive Abilities T-Scores | 51.9 ± 7.2 | 51.6 ± 8.8 | 52 ± 8.4 | 51.3 ± 12.2 |
| Wellbeing Aspect | Pre-CG | Pre-PG | Post-CG | Post-PG |
|---|---|---|---|---|
| Autonomy | 17.1 ± 3 | 16 ± 3 | 16.6 ± 2.7 | 15.7 ± 3.6 |
| Environmental Mastery | 16.1 ± 2.8 | 15.1 ± 3.6 | 15.1 ± 3.8 | 15.5 ± 3.6 |
| Personal Growth | 20.1 ± 1.2 | 20.3 ± 1 | 19 ± 2.2 | 19.4 ± 2.3 |
| Positive Relation with Others | 17.3 ± 3.1 | 18.1 ± 2.8 | 16.8 ± 3 | 16.3 ± 3.9 |
| Purpose in Life | 17.4 ± 2.6 | 17.7 ± 2.1 | 16.4 ± 3 | 16.5 ± 3.9 |
| Self-Acceptance | 17.6 ± 2.7 | 17.8 ± 3.6 | 17.13 ± 2.4 | 17.3 ± 3.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flores, V.A.; Kisiolek, J.N.; Ramani, A.; Townsend, R.; Rodriguez, E.; Butler, B.; Stewart, L.K. Effects of Oral Cannabidiol on Health and Fitness in Healthy Adults: An 8-Week Randomized Trial. Nutrients 2023, 15, 2664. https://doi.org/10.3390/nu15122664
Flores VA, Kisiolek JN, Ramani A, Townsend R, Rodriguez E, Butler B, Stewart LK. Effects of Oral Cannabidiol on Health and Fitness in Healthy Adults: An 8-Week Randomized Trial. Nutrients. 2023; 15(12):2664. https://doi.org/10.3390/nu15122664
Chicago/Turabian StyleFlores, Victoria A., Jacob N. Kisiolek, Arjun Ramani, Ryland Townsend, Edwin Rodriguez, Blake Butler, and Laura K. Stewart. 2023. "Effects of Oral Cannabidiol on Health and Fitness in Healthy Adults: An 8-Week Randomized Trial" Nutrients 15, no. 12: 2664. https://doi.org/10.3390/nu15122664