
Development and Pilot Testing of Smartphone-Based Hearing Test Application


Abstract
:1. Introduction
- Unlike other smartphone-based screening applications, the proposed smartphone application can quantify the hearing threshold levels within clinically accepted standards for NH people.
- We propose a novel subjective test-based approach to calibrate a smartphone-earphone combination with respect to the reference audiometer.
- In PTA, we use continuous tones that are different from regular short interval tones. The advantages of using continuous tones are that they minimize harmonic distortions and do not require the attention of the user.
2. Participants and Equipment
2.1. Participants
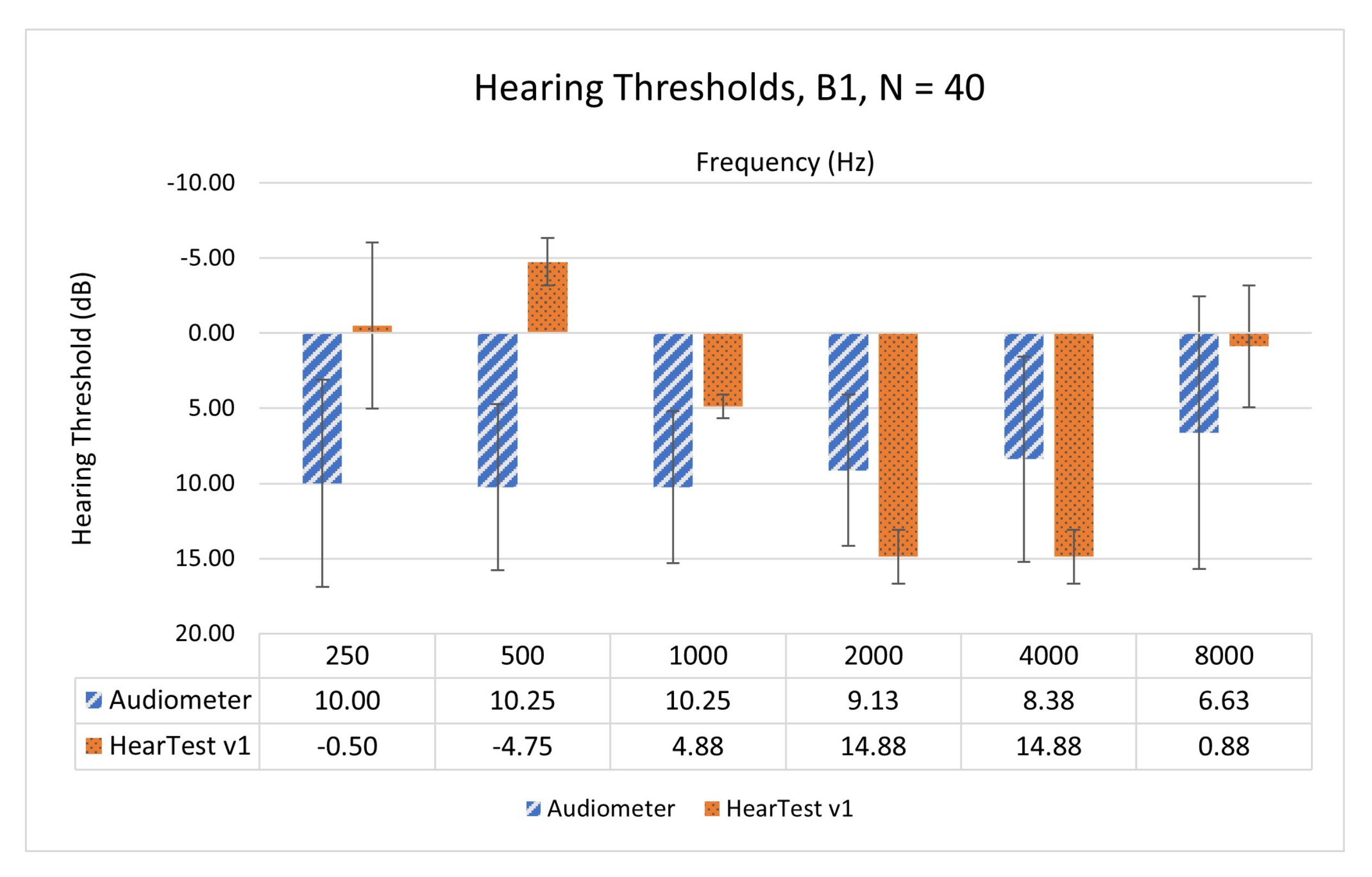
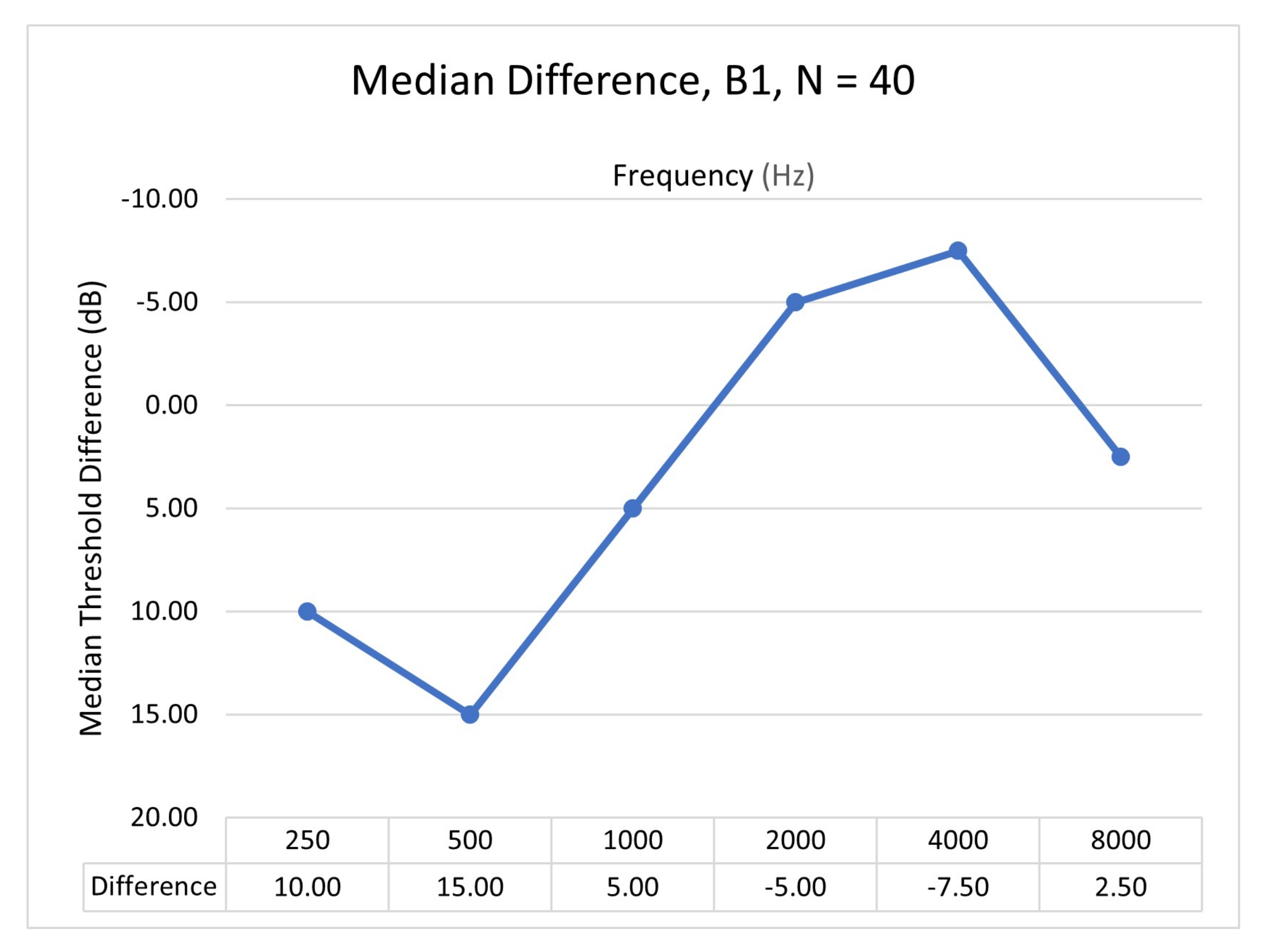
- Subjective test batch 1 (B1): For the first version of the application, a total of 20 participants self-identified as having NH ranging from ages 19 to 28 years with mean and standard deviation as , except for 2 participants, aged 52 and 56, were recruited. Out of 20, the male and female count was 7 and 13, respectively.
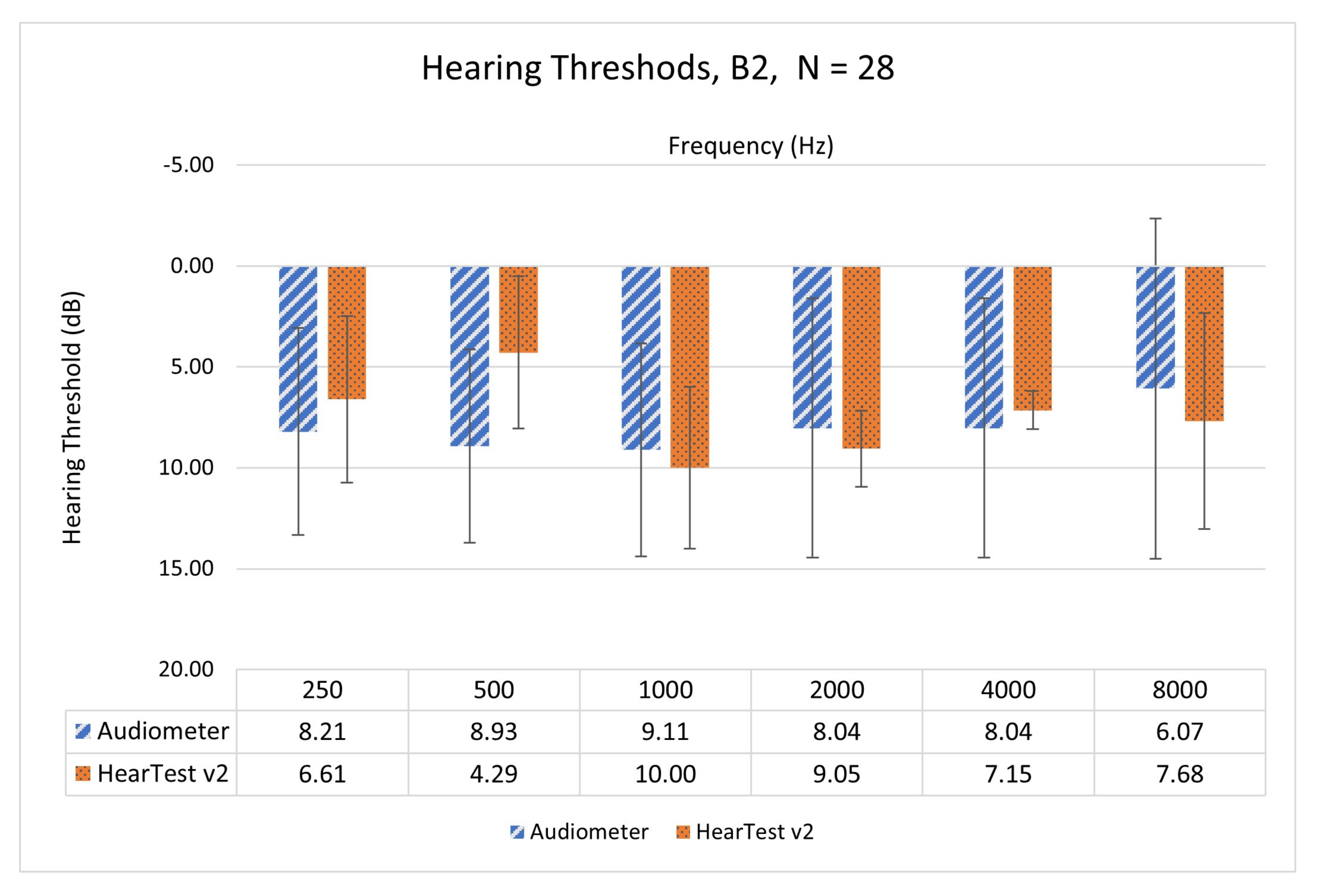
- Subjective test batch 2 (B2): A total of 14 participants also self-identified as having NH ranging from ages 20 to 30 years with mean and standard deviation as were recruited for a further hearing test with application version 2 (HearTest v2). Out of 14, the male and female count was 4 and 10, respectively.
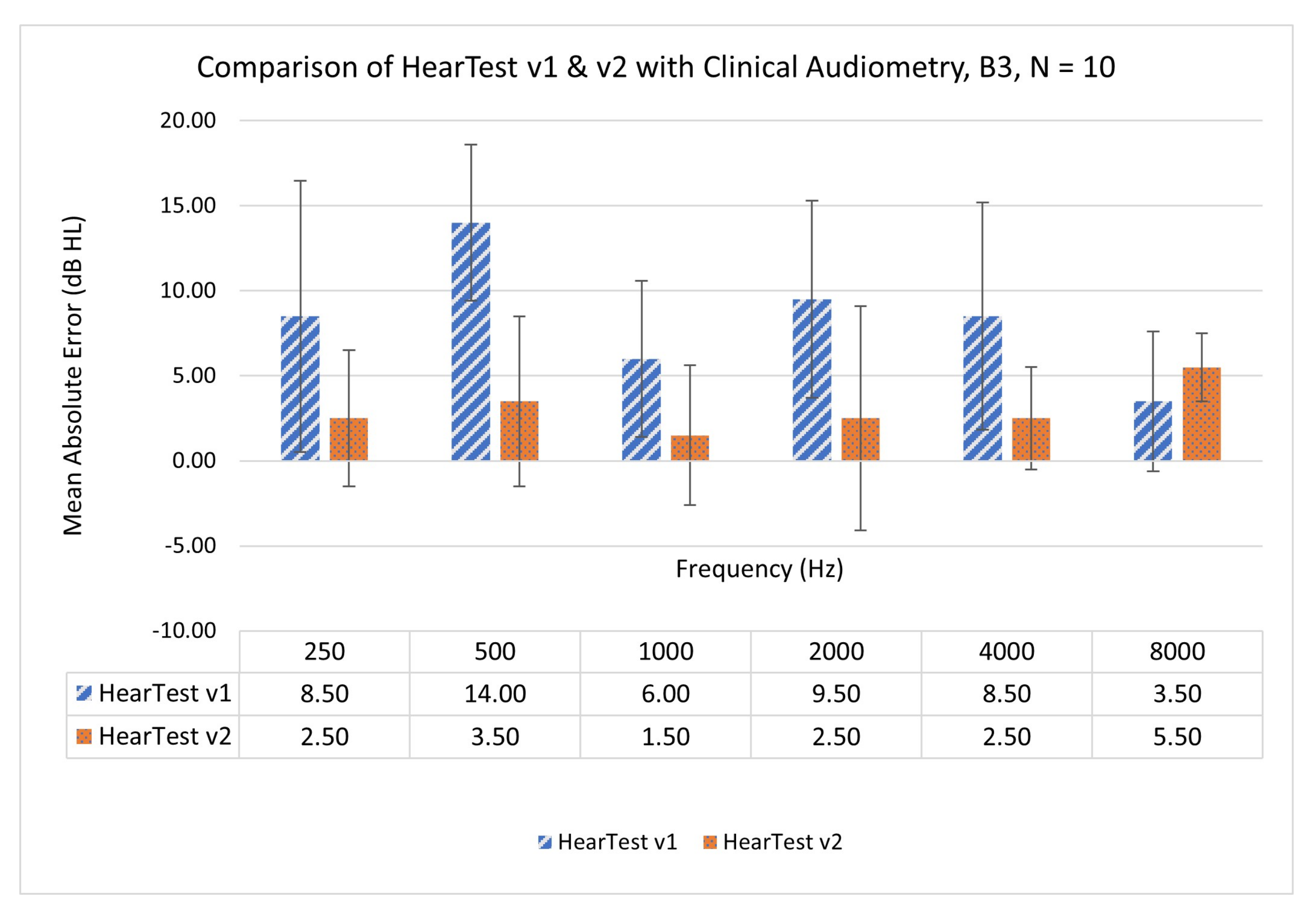
- Subjective test batch 3 (B3): five participants from B1 were again called for retesting with the HearTest v2.
2.2. Test Procedure and Equipment
3. Methodology
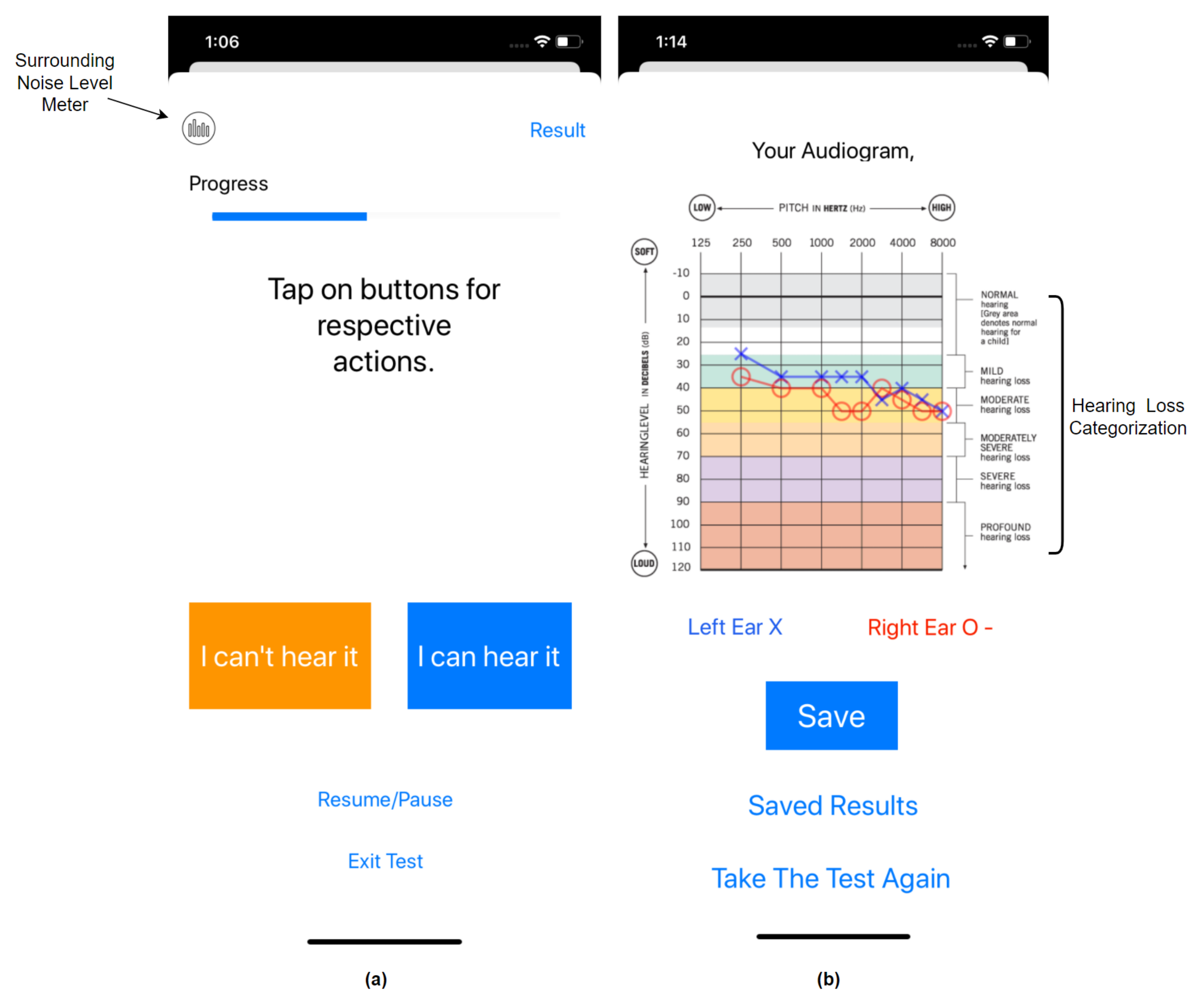
4. Smartphone Application
5. Calibration
6. Results
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NH | Normal hearing |
| SPL | Sound pressure level |
| HL | Hearing level |
| RETSPL | Reference equivalent threshold SPL |
| HI | Hearing-impaired |
| TE | Testing ear |
| NTE | Non-testing ear |
References
- World Health Organization. Hearing Loss Fact Sheet. 2021. Available online: who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss (accessed on 11 January 2021).
- Hearing Loss Association of America. 2021. Available online: https://www.hearingloss.org/ (accessed on 11 January 2021).
- Phatak, S.A.; Yoon, Y.S.; Gooler, D.M.; Allen, J.B. Consonant recognition loss in hearing impaired listeners. J. Acoust. Soc. Am. 2009, 126, 2683–2694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, K.; Panahi, I.M. Frequency-based multi-band adaptive compression for hearing aid application. Proc. Meet. Acoust. 2019, 39, 055004. [Google Scholar]
- Bhat, G.S.; Shankar, N.; Reddy, C.K.; Panahi, I.M. A real-time convolutional neural network based speech enhancement for hearing impaired listeners using smartphone. IEEE Access 2019, 7, 78421–78433. [Google Scholar] [CrossRef] [PubMed]
- Bhat, G.S.; Shankar, N.; Panahi, I.M. Design and Integration of alert signal detector and separator for hearing Aid applications. IEEE Access 2020, 8, 106296–106309. [Google Scholar] [CrossRef]
- Patel, K.; Panahi, I.M. Compression Fitting of Hearing Aids and Implementation. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 968–971. [Google Scholar]
- Shankar, N.; Bhat, G.S.; Panahi, I. Comparison and real-time implementation of fixed and adaptive beamformers for speech enhancement on smartphones for hearing study. In Proceedings of the Meetings on Acoustics 178ASA, San Diego, CA, USA, 2–6 December 2019; Volume 39. [Google Scholar]
- Küçük, A.; Ganguly, A.; Hao, Y.; Panahi, I.M. Real-Time Convolutional Neural Network-Based Speech Source Localization on Smartphone. IEEE Access 2019, 7, 169969–169978. [Google Scholar] [CrossRef]
- Patel, K.; Panahi, I.M. Efficient Real-Time Acoustic Feedback Cancellation using Adaptive Noise Injection Algorithm. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 972–975. [Google Scholar]
- Davis, A.C.; Hoffman, H.J. Hearing loss: Rising prevalence and impact. Bull. World Health Organ. 2019, 97, 646. [Google Scholar] [CrossRef]
- Olusanya, B.O. Early Hearing Detection and Intervention in Developing Countries: Current Status and Prospects. Volta Rev. 2006, 106, 381–418. [Google Scholar] [CrossRef]
- Jayawardena, A.; Waller, B.; Edwards, B.; Larsen-Reindorf, R.; Esinam Anomah, J.; Frimpong, B.; Gina, A.; Netterville, J.; Saunders, J.; Basura, G.J.; et al. Portable audiometric screening platforms used in low-resource settings: A review. J. Laryngol. Otol. 2019, 133, 74–79. [Google Scholar] [CrossRef]
- Colsman, A.; Supp, G.G.; Neumann, J.; Schneider, T.R. Evaluation of Accuracy and Reliability of a Mobile Screening Audiometer in Normal Hearing Adults. Front. Psychol. 2020, 11, 744. [Google Scholar] [CrossRef]
- Barczik, J.; Serpanos, Y.C. Accuracy of smartphone self-hearing test applications across frequencies and earphone styles in adults. Am. J. Audiol. 2018, 27, 570–580. [Google Scholar] [CrossRef]
- Peer, S.; Fagan, J.J. Hearing loss in the developing world: Evaluating the iPhone mobile device as a screening tool. S. Afr. Med. J. 2015, 105, 35–39. [Google Scholar] [CrossRef] [Green Version]
- Margolis, R.H.; Morgan, D.E. Automated pure-tone audiometry: An analysis of capacity, need, and benefit. Am. J. Audiol. 2008, 17, 109–113. [Google Scholar] [CrossRef]
- Handzel, O.; Ben-Ari, O.; Damian, D.; Priel, M.M.; Cohen, J.; Himmelfarb, M. Smartphone-based hearing test as an aid in the initial evaluation of unilateral sudden sensorineural hearing loss. Audiol. Neurotol. 2013, 18, 201–207. [Google Scholar] [CrossRef]
- Bright, T.; Pallawela, D. Validated smartphone-based apps for ear and hearing assessments: A review. JMIR Rehabil. Assist. Technol. 2016, 3, e13. [Google Scholar] [CrossRef] [Green Version]
- Van Tonder, J.; Swanepoel, D.W.; Mahomed-Asmail, F.; Myburgh, H.; Eikelboom, R.H. Automated smartphone threshold audiometry: Validity and time efficiency. J. Am. Acad. Audiol. 2017, 28, 200–208. [Google Scholar] [CrossRef] [Green Version]
- Szudek, J.; Ostevik, A.; Dziegielewski, P.; Robinson-Anagor, J.; Gomaa, N.; Hodgetts, B.; Ho, A.; Mathers, C.; Smith, A.; Concha, M.; et al. Can Uhear me now? Validation of an iPod-based hearing loss screening test. J. Otolaryngol. Head Neck Surg. 2012, 41, S78. [Google Scholar]
- Foulad, A.; Bui, P.; Djalilian, H. Automated audiometry using apple iOS-based application technology. Otolaryngol. Head Neck Surg. 2013, 149, 700–706. [Google Scholar] [CrossRef] [Green Version]
- Khoza-Shangase, K.; Kassner, L. Automated screening audiometry in the digital age: Exploring uhear (tm) and its use in a resource-stricken developing country. Int. J. Technol. Assess. Health Care 2013, 29, 42. [Google Scholar] [CrossRef]
- Abu-Ghanem, S.; Handzel, O.; Ness, L.; Ben-Artzi-Blima, M.; Fait-Ghelbendorf, K.; Himmelfarb, M. Smartphone-based audiometric test for screening hearing loss in the elderly. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 333–339. [Google Scholar] [CrossRef]
- Chen, F.; Wang, S.; Li, J.; Tan, H.; Jia, W.; Wang, Z. Smartphone-based hearing self-assessment system using hearing aids with fast audiometry method. IEEE Trans. Biomed. Circuits Syst. 2018, 13, 170–179. [Google Scholar] [CrossRef]
- Yao, J.; Wan, Y.; Givens, G. Design of a web services based system for remote hearing diagnosis. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 5215–5218. [Google Scholar]
- Ho, C.Y.; Li, P.C.; Young, S.T. Reference equivalent threshold sound pressure levels for Apple EarPods. J. Acoust. Soc. Am. 2017, 141, EL115–EL119. [Google Scholar] [CrossRef] [Green Version]
- Burk, M.H.; Wiley, T.L. Continuous versus pulsed tones in audiometry. Am. J. Audiol. 2004, 13, 54–61. [Google Scholar] [CrossRef]
- ASHA—American Speech-Language Hearing Association. Degree of Hearing Loss. 2021. Available online: https://www.asha.org/public/hearing/Degree-of-Hearing-Loss/ (accessed on 11 January 2021).
- Smartphone-Based Hearing Test, iOS Application. Available online: https://github.com/ssprl/Smartphone-based-Audiometry (accessed on 11 January 2021).
- Acoustical Society of America. American National Standard Acoustical Terminology; American National Standards Institute (ANSI): New York, NY, USA, 2006. [Google Scholar]
- Weissler, P.G. International standard reference zero for audiometers. J. Acoust. Soc. Am. 1968, 44, 264–275. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Han, W. Sound pressure levels generated at risk volume steps of portable listening devices: Types of smartphone and genres of music. BMC Public Health 2018, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Masalski, M.; Kipiński, L.; Grysiński, T.; Kręcicki, T. Hearing tests on mobile devices: Evaluation of the reference sound level by means of biological calibration. J. Med Internet Res. 2016, 18, e130. [Google Scholar] [CrossRef] [PubMed]
- Studebaker, G.A. Clinical masking of the nontest ear. J. Speech Hear. Disord. 1967, 32, 360–371. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.; Chasin, M.; English, K.M.; Hood, L.J.; Tillery, K.L. Handbook of Clinical Audiology; Williams & Wilkins Baltimore: Baltimore, MD, USA, 1978; Volume 428. [Google Scholar]
- Chaiklin, J.B. Inter aural attenuation and cross-hearing in air-conduction audiometry. J. Aud. Res. 1967, 7, 413–424. [Google Scholar]
- Snyder, J.M. Interaural attenuation characteristics in audiometry. Laryngoscope 1973, 83, 1847–1855. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 250 | 500 | 1000 | 2000 | 4000 | 8000 | |
|---|---|---|---|---|---|---|
| ER 3A | 14.5 | 6.0 | 0 | 2.5 | 0 | −3.5 |
| HearTest v1 | 11.8 | 9.5 | 6 | 2.3 | 6.7 | 16.2 |
| HearTest v2 | 1.8 | −5.5 | 1 | 7.3 | 13.7 | 13.7 |
| Smartphone | Channel | 250 | 500 | 1000 | 2000 | 4000 | 8000 |
|---|---|---|---|---|---|---|---|
| iPhone XR | L | 85.1 | 93.5 | 107.2 | 112.8 | 106 | 108.8 |
| R | 84.9 | 93.4 | 107.3 | 113 | 106.1 | 108.7 | |
| iPhone 10 | L | 83.4 | 94.6 | 107.8 | 113.5 | 105.7 | 108.6 |
| R | 83.5 | 94.1 | 108.1 | 113.2 | 105.8 | 108.2 | |
| iPhone 8 | L | 83.1 | 93.3 | 107.3 | 112.8 | 106.4 | 108.5 |
| R | 83.3 | 93.3 | 107.2 | 112.7 | 106.1 | 108.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, K.; Thibodeau, L.; McCullough, D.; Freeman, E.; Panahi, I. Development and Pilot Testing of Smartphone-Based Hearing Test Application. Int. J. Environ. Res. Public Health 2021, 18, 5529. https://doi.org/10.3390/ijerph18115529
Patel K, Thibodeau L, McCullough D, Freeman E, Panahi I. Development and Pilot Testing of Smartphone-Based Hearing Test Application. International Journal of Environmental Research and Public Health. 2021; 18(11):5529. https://doi.org/10.3390/ijerph18115529
Chicago/Turabian StylePatel, Kashyap, Linda Thibodeau, David McCullough, Emma Freeman, and Issa Panahi. 2021. "Development and Pilot Testing of Smartphone-Based Hearing Test Application" International Journal of Environmental Research and Public Health 18, no. 11: 5529. https://doi.org/10.3390/ijerph18115529