





Abstract
Guillain-Barré syndrome (GBS) is the most common cause of acute flaccid paralysis worldwide, and is thought to be immune-mediated. It is preceded by upper respiratory or gastrointestinal infection in about two-thirds of cases and is associated with some viral infections, including influenza. GBS has also been associated with the 1976 swine-influenza vaccine. Thereafter, some studies have shown a small increased risk of GBS following receipt of seasonal and 2009 H1N1 monovalent influenza vaccines. Studies over the years have also shown an increased risk of GBS following influenza infection, and the magnitude of risk is several times greater than that following influenza vaccination. Because GBS is rare, and even rarer following vaccination, it is difficult to estimate precise risk. We try to shed light on the complex relationship of GBS and its association with influenza and influenza vaccines over the past 35 years.
Guillain-Barré syndrome (GBS) came to the forefront during the 1976 swine influenza vaccination program when an increased risk was found following vaccination [1]. Thirty-five years later we are still grappling with this increased risk; concerns continue that the risk observed in 1976 might surface again following administration of influenza vaccines, which have a change in the strain nearly every year [2]. These concerns have led to many studies assessing this risk, especially, because in the United States, annual influenza vaccine is now recommended for everyone aged ≥6 months [2]. In this review, we purport that there may be enough evidence in 2013 to be somewhat reassured to move past the fear that influenza vaccines can cause GBS of the same magnitude that was described in The Swine Flu Affair [3].
GUILLAIN-BARRÉ SYNDROME
GBS is the most common cause of acute flaccid paralysis worldwide now that poliomyelitis is nearly eradicated. It results from damage to the peripheral nerves and nerve roots, presenting with progressive bilateral symmetric weakness of the lower limbs over a period of 12 hours and reaching a plateau at approximately 28 days. The onset of symptoms in about two-thirds of the cases is preceded by an upper respiratory or gastrointestinal infection. Most patients completely recover, although there is about a 5% case-mortality rate [4, 5].
The annual incidence of GBS is 0.4–4.0 cases per 100 000 population among all ages. In children and adolescents, the range is 0.4–1.5 cases per 100 000 and then the incidence increases throughout adulthood to about 4.0 cases per 100 000 after age 75 years [6–8]. GBS is thought to be immune-mediated, in which antibodies in response to an antigenic stimulus, such as a bacterial or viral infection, cross-react with nerve ending antigens; this is often referred to as molecular mimicry. Infection preceding GBS is quite common, but the specific infectious agent is unknown in 60% of the cases. Several infectious agents have been shown to be associated with GBS, most notably Campylobacter jejuni [9–13].
GBS AND INFLUENZA VACCINES
GBS became a major vaccine safety concern in 1976 when there was a threat of a swine-origin influenza pandemic and the United States government initiated a national vaccination program. After approximately 45 million people were vaccinated with influenza A/New Jersey/1976 vaccine, an increased number of postvaccination GBS cases were reported. Investigations revealed up to a 8-fold increased risk of GBS following receipt of the 1976 influenza vaccine; the risk was found to be highest 2–3 weeks after vaccination. The attributable risk was estimated at 1 additional case of GBS for every 100 000 doses administered [1, 14]. As a result of this adverse outcome following vaccination, as well as the fact that the pandemic never materialized, the 1976 influenza vaccination program was halted [3]. Nearly 30 years later, in 2004, the Institute of Medicine (IOM) reviewed the evidence regarding the association of GBS with the 1976 swine influenza vaccine and concluded that “the evidence favors acceptance of a causal relationship between 1976 swine influenza vaccines and GBS in adults” [15].
Since 1976, several published studies have assessed risk of GBS following receipt of seasonal inactivated influenza vaccines. Most studies did not demonstrate a significant association between seasonal influenza vaccine and GBS, and most point estimates were not significant (Figure 1) [16–23]. However, 2 studies reporting positive findings garnered much attention. In 2006, Juurlink et al studied the association of GBS with influenza vaccines administered during 1992–2004 in Canada; using a self-controlled case series design, they found a small but significant increased risk of GBS in the 6 weeks following receipt of influenza vaccine (relative risk [RR] 1.45; 95% confidence interval [CI], 1.05–1.99) [20]. The other notable study used US data from the period 1992–1994 (2 influenza seasons) and demonstrated an overall increased RR of 1.7 (95% CI, 1.0–2.8; P = .04), although an increased risk was not demonstrated when using data from each influenza season separately [22]. The RR of 1.7 suggests slightly more than 1 additional case of GBS per million persons vaccinated against influenza. Based on evidence from these 2 studies, a risk estimate of 1 additional GBS case per 1 million persons vaccinated has been communicated to the public and found in the Advisory Committee on Immunization Practices recommendations and the Vaccine Information Statements for influenza vaccines [2, 24]. The IOM reviewed evidence accumulated after 1976 through 2008 and concluded that “the evidence is inadequate to accept or reject a causal relationship between influenza vaccine and GBS.” The IOM further concluded that the evidence was not adequate because of potential confounding due to season and influenza infection and also because each year the influenza strains included in the vaccine typically differ [25].
More recently, GBS risk assessment following influenza vaccination once again came to the forefront. During the 2009 H1N1 influenza pandemic, vaccine safety surveillance was heightened and critical to the unadjuvanted 2009 monovalent inactivated influenza A(H1N1) (2009 pH1N1 vaccine) vaccination program that began in October 2009. GBS was a particularly important component of the pandemic response, because the 1976 swine-origin influenza vaccine was associated with an increased risk of GBS and the 2009 H1N1 influenza virus was also of swine origin, and there was a high degree of public interest regarding the safety of pandemic H1N1 vaccines. In the United States, several federal agencies enhanced, adapted, or created surveillance systems to monitor 2009 pH1N1 vaccine safety including assessing the risk of GBS following vaccination [26]. The results of surveillance from most of these systems are captured in Table 1. At the Centers for Disease Control and Prevention (CDC), active GBS case-finding surveillance using a population catchment of nearly 45 million people was implemented as part of the Emerging Infections Program (EIP), a long-standing collaboration with the CDC, local health departments, academic institutions, healthcare providers, specialist networks, and clinical laboratories [27]. In November 2009, prospective cohort analyses showed a small increased risk of GBS within the 6 weeks following vaccination and an attributable risk of approximately 1 additional case of GBS per million persons vaccinated [28]. Final analyses confirmed this small increased risk within 6 weeks of vaccination [29, 30]. The CDC's Vaccine Safety Datalink, a population-based database linking vaccine data with health outcome data, also found a significant increased risk of GBS [31] in the primary self-controlled analysis, and, although the surveillance from the Food and Drug Administration did not demonstrate a statistically significant finding, the RR point estimate was elevated [32]. To increase the power to assess an increased risk of this rare disease, a meta-analysis combined data on 23 million persons vaccinated from all the federal systems that participated in 2009 pH1N1 vaccine safety monitoring. Consistent with previous studies assessing the seasonal influenza vaccine data from earlier years [20, 22], this pooled analysis found an attributable risk of 1–3 additional GBS cases per million persons vaccinated with pH1N1 [33] (Table 1). Findings from European studies assessing the risk of GBS following the 2009 pH1N1 vaccines somewhat differed from what was observed in the United States. A multicountry case-control study using data from several European countries, where predominately adjuvanted pH1N1 vaccines were used, found no increased risk for GBS within 6 weeks of vaccination after adjusting for influenza-like illness (ILI)/upper respiratory tract infection (URTI) and seasonal influenza vaccination [34]. The United Kingdom also primarily used adjuvanted vaccines and found no increased risk using a self-controlled case series design (RR = 1.05; 95% CI, .37–2.24) [35]. In addition, a large international study found a significant increased risk of GBS following the 2009 pH1N1 vaccines (relative incidence [RI] = 2.33; 95% CI, 1.5–3.6); however, when stratifying by vaccine type (adjuvanted or unadjuvanted), the RI for the unadjuvanted group was significantly increased (RI = 3.1; 95% CI, 1.7–5.7) and higher than that for the adjuvanted group (RI = 1.7; 95% CI, .9–3.3) [36]. Finally, a study from Quebec, Canada, found an attributable risk of 2 additional cases of GBS per million doses administered, similar to the US surveillance findings; however, Quebec primarily used adjuvanted H1N1 vaccines. The authors noted that the excess risk was only found in persons aged >50 years [37]. Results of these studies from the United States, Europe, Canada, and internationally gave mixed results but in general suggest an increased risk of GBS after either adjuvanted or unadjuvanted vaccine.
2009 Monovalent Inactivated Influenza A(H1N1) Vaccine and Guillain-Barré Syndrome, US Vaccine Safety Surveillance, 2009–2010
| Data Source [Reference] | Study Designa | Final Analysis RR/OR (95% CI) | ARb |
|---|---|---|---|
| Emerging Infections Program (CDC) Wise et al [30] | Unvaccinated controlc | 1.57 (1.02–2.21) (all ages) | 1.2 |
| 1.67 (.58–3.22) (<25 y) | |||
| 1.54 (.90–2.25) (≥25 y) | |||
| Tokars et al [29] | Self-controlled | 2.1 (1.2–3.5) (all ages) | 1–3 |
| 3.0 (1.0–9.1) (6 mo–24 y) | |||
| Vaccine Safety Datalink (CDC) Greene et al [31] | Self-controlled | 4.4 (1.3–14.2) | 5 |
| Case-centered | 2.0 (.5–8.1) | ||
| PRISM (FDA) Yih et al [32] | Self-controlled | 2.50 (.42–15.0) | |
| Case-centered | 1.15 (.07–18.6) | ||
| Meta-analysisd Salmon et al [33] | Self-controlled | 2.35 (1.42–4.01) (all ages) | 1.6 |
| 2.33 (.65–10.5) (<18 y) |
| Data Source [Reference] | Study Designa | Final Analysis RR/OR (95% CI) | ARb |
|---|---|---|---|
| Emerging Infections Program (CDC) Wise et al [30] | Unvaccinated controlc | 1.57 (1.02–2.21) (all ages) | 1.2 |
| 1.67 (.58–3.22) (<25 y) | |||
| 1.54 (.90–2.25) (≥25 y) | |||
| Tokars et al [29] | Self-controlled | 2.1 (1.2–3.5) (all ages) | 1–3 |
| 3.0 (1.0–9.1) (6 mo–24 y) | |||
| Vaccine Safety Datalink (CDC) Greene et al [31] | Self-controlled | 4.4 (1.3–14.2) | 5 |
| Case-centered | 2.0 (.5–8.1) | ||
| PRISM (FDA) Yih et al [32] | Self-controlled | 2.50 (.42–15.0) | |
| Case-centered | 1.15 (.07–18.6) | ||
| Meta-analysisd Salmon et al [33] | Self-controlled | 2.35 (1.42–4.01) (all ages) | 1.6 |
| 2.33 (.65–10.5) (<18 y) |
Abbreviations: AR, attributable risk; CDC, Centers for Disease Control and Prevention; CI, confidence interval; FDA, Food and Drug Administration; OR, odds ratio; PRISM, Postlicensure Rapid Immunization Safety Monitoring; RR, relative risk.
a All cases confirmed through medical records review.
b Per million doses administered.
c Includes person-time for vaccinated cases that occurred >6 weeks following vaccination.
d Includes data from the Emerging Infections Program, Vaccine Safety Datalink, PRISM, Department of Veterans Affairs, Centers for Medicare and Medicaid Services, and Department of Defense.
2009 Monovalent Inactivated Influenza A(H1N1) Vaccine and Guillain-Barré Syndrome, US Vaccine Safety Surveillance, 2009–2010
| Data Source [Reference] | Study Designa | Final Analysis RR/OR (95% CI) | ARb |
|---|---|---|---|
| Emerging Infections Program (CDC) Wise et al [30] | Unvaccinated controlc | 1.57 (1.02–2.21) (all ages) | 1.2 |
| 1.67 (.58–3.22) (<25 y) | |||
| 1.54 (.90–2.25) (≥25 y) | |||
| Tokars et al [29] | Self-controlled | 2.1 (1.2–3.5) (all ages) | 1–3 |
| 3.0 (1.0–9.1) (6 mo–24 y) | |||
| Vaccine Safety Datalink (CDC) Greene et al [31] | Self-controlled | 4.4 (1.3–14.2) | 5 |
| Case-centered | 2.0 (.5–8.1) | ||
| PRISM (FDA) Yih et al [32] | Self-controlled | 2.50 (.42–15.0) | |
| Case-centered | 1.15 (.07–18.6) | ||
| Meta-analysisd Salmon et al [33] | Self-controlled | 2.35 (1.42–4.01) (all ages) | 1.6 |
| 2.33 (.65–10.5) (<18 y) |
| Data Source [Reference] | Study Designa | Final Analysis RR/OR (95% CI) | ARb |
|---|---|---|---|
| Emerging Infections Program (CDC) Wise et al [30] | Unvaccinated controlc | 1.57 (1.02–2.21) (all ages) | 1.2 |
| 1.67 (.58–3.22) (<25 y) | |||
| 1.54 (.90–2.25) (≥25 y) | |||
| Tokars et al [29] | Self-controlled | 2.1 (1.2–3.5) (all ages) | 1–3 |
| 3.0 (1.0–9.1) (6 mo–24 y) | |||
| Vaccine Safety Datalink (CDC) Greene et al [31] | Self-controlled | 4.4 (1.3–14.2) | 5 |
| Case-centered | 2.0 (.5–8.1) | ||
| PRISM (FDA) Yih et al [32] | Self-controlled | 2.50 (.42–15.0) | |
| Case-centered | 1.15 (.07–18.6) | ||
| Meta-analysisd Salmon et al [33] | Self-controlled | 2.35 (1.42–4.01) (all ages) | 1.6 |
| 2.33 (.65–10.5) (<18 y) |
Abbreviations: AR, attributable risk; CDC, Centers for Disease Control and Prevention; CI, confidence interval; FDA, Food and Drug Administration; OR, odds ratio; PRISM, Postlicensure Rapid Immunization Safety Monitoring; RR, relative risk.
a All cases confirmed through medical records review.
b Per million doses administered.
c Includes person-time for vaccinated cases that occurred >6 weeks following vaccination.
d Includes data from the Emerging Infections Program, Vaccine Safety Datalink, PRISM, Department of Veterans Affairs, Centers for Medicare and Medicaid Services, and Department of Defense.
Although an increased risk of GBS following 2009 pH1N1 vaccines was reported in most of the US studies, it is perplexing that vaccine safety surveillance in the United States during the years since the 2009 pandemic (2010–2011, 2011–2012, and 2012–2013 influenza seasons) did not find a signal for an increased risk of GBS (CDC, personal communication), yet in all 3 years the influenza vaccines included the 2009 pH1N1 strain. In addition, in 2009–2010, 27.0% of the US population aged ≥6 months received the 2009 pH1N1vaccines. The coverage was 43.0%, 42.0%, and 45.0% in the next 3 seasons, respectively [38]. Because an increasing number of individuals received influenza vaccines that included the same 2009 pH1N1 strain, it is reasonable to ask why we did not see an increase risk of GBS following vaccination in the subsequent years. What had changed? Among other things, there were 2 major differences: the lack of nationally representative, large population–based and comprehensive surveillance activities for GBS case finding [27] and very low influenza illness during subsequent seasons compared with that of 2009–2010 [39].
GBS AND INFLUENZA
Even before the term “Guillain-Barré syndrome” was in use in clinical medicine, postinfectious polyneuritis cases had been reported since the 1918–1920 Spanish influenza pandemic [9]. Although URTI has been known to precede GBS, specific association between influenza infection and GBS has only started to be reported more recently. Studies from the United Kingdom in 2007 and 2009 demonstrated a strong association with influenza. Tam et al found an odds ratio (OR) of 18.6 (95% CI, 7.5–46.4) for GBS occurring within 60 days of ILI [40], and Stowe et al, using a self-controlled case series design, found an RR of 7.35 (95% CI, 4.36–12.38) for GBS occurring within 90 days of an ILI [23]. These 2 studies used the same primary care database, but the Stowe et al analysis used 5 more years of data (1990–2005 vs 1991–2001). Stowe et al also used a 90-day risk period following exposure, whereas Tam et al used a 60-day period of increased risk, which may have accounted for the higher magnitude of risk found in Tam et al's analysis; earlier studies found that the risk for GBS was greatest 2–3 weeks following an exposure but that increased risk continued through 6–8 weeks [1]. Another study used time-series analyses demonstrating a positive association between GBS hospital admissions and laboratory-confirmed influenza cases [12].
Studies during the 2009 H1N1 pandemic also support an increased risk of GBS following 2009 pH1N1 infection. A brief report by Verity et al described the GBS cases reported by pediatricians during an active surveillance program implemented specifically during the 2009 H1N1 pandemic [41]. From September 2009 through August 2010, 57 children were reported with a diagnosis of GBS, and 49 of the 57 children had clinical or laboratory evidence of infection within the 3 months prior to GBS onset; 9 of these were laboratory-confirmed influenza. Only 1 child had received the pH1N1 vaccine within 6 weeks of GBS, which, based on GBS background incidence for children, was expected by chance alone. Furthermore, the peak of the second wave of the H1N1 pandemic occurred just prior to a notable increase in reported GBS cases among children [41]. Other studies assessing the risk of GBS following the 2009 pH1N1 vaccines, such as the Greene et al study in the United States and in the European pooled analysis [31, 34], both described above, suggested that the findings may have been confounded by influenza illness that peaked just as the vaccines became available and widely distributed (Figure 2). In a secondary analysis (case-centered), Greene et al, controlling for seasonality, which indirectly controls for influenza illness, found that the increased risk for GBS observed in the primary analysis decreased and was no longer significant (OR = 2.0; 95% CI, .5–8.1) (Table 1) [31]. The results from the European pooled data, before adjustment for ILI and URTI, demonstrated a significant OR of 2.8 (95% CI, 1.3–6.0), but after adjustment, the increased risk estimate disappeared (OR = 1.0; 95% CI, .3–2.7) [42].1
![Risk estimates (with 95% confidence intervals) of Guillain-Barré syndrome following influenza vaccines in adults, select studies, 1979–2008. *Included separate estimates for 2000 and 2001. **Included separate estimates for 3 influenza seasons: 2005–2006, 2006–2007, and 2007–2008; sequential analyses do not include confidence intervals. Select studies: Greene et al [18], Burwen et al [17], Baxter R et al [16], Juurlink et al [20], Hughes et al [19], Lasky et al [22], Stowe et al [23], and Kaplan et al [21].](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/cid/58/8/10.1093/cid/ciu005/2/m_ciu00501.jpeg?Expires=1716398874&Signature=zXcdUNEbY0Md~mZEndn~RwR7aOLTZAcedIwz702QlKQB7StcVG~Q-6NLTFn-i7VqNaWPPo3ebiGvDH7alCXKbC7TRldYkohTlHYWasIFeabYZ2BbMIZnvqoQWlUCiiH87NNIURq~1P0rm3OqC5gCzn6lqd0-PL4asaJDxTrAIikjF5bN4vHuCZ8E5FWWToyXq4d0cvamSaqogit~CelbAmllHkLRF1KspBwSYJxQg-MegyZYIUrt~8-YWw4SlyMQ5G1X3MSwKNqiiPiXe3SutObXsIh3~XrDa1jkoJHhsqsSIYogUGetbfyXuMtyAhO-1YUvb-fSAvXdHyAvQqT6HA__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Risk estimates (with 95% confidence intervals) of Guillain-Barré syndrome following influenza vaccines in adults, select studies, 1979–2008. *Included separate estimates for 2000 and 2001. **Included separate estimates for 3 influenza seasons: 2005–2006, 2006–2007, and 2007–2008; sequential analyses do not include confidence intervals. Select studies: Greene et al [18], Burwen et al [17], Baxter R et al [16], Juurlink et al [20], Hughes et al [19], Lasky et al [22], Stowe et al [23], and Kaplan et al [21].
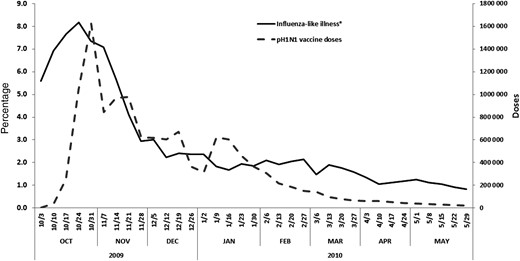
Percentage of influenza-like illnesses (ILIs) and 2009 pH1N1 vaccinations in the Emerging Infections Program (EIP) by week (weeks ending in corresponding dates), United States, October 2009–May 2010. *Weekly percentage of outpatient visits for ILI among ILINet sentinel physicians in the EIP catchment area.
GBS, INFLUENZA, AND INFLUENZA VACCINE
The observed increased risk for GBS following influenza vaccination after 1976 has primarily come from studies completed during the 2009 H1N1 pandemic. However, the 2009 H1N1 pandemic and the 2009–2010 influenza vaccine program were unique in that there was little or no nonpandemic influenza virus strain circulating and the peak circulation of the 2009 H1N1 pandemic virus was much earlier (October 2009) than typical influenza seasons (usually January–February). Furthermore, 2009 pH1N1 vaccines became available and widely distributed at the same time the 2009 H1N1 pandemic peaked (Figure 2).
In an attempt to determine any confounding due to the simultaneous circulation of wild-type 2009 pH1N1 influenza and administration of 2009 pH1N1 vaccines, data from the CDC EIP active GBS case-finding surveillance collected from October 2009 through May 2010 was reanalyzed using a different approach. Rather than assessing the increased risk of GBS during the 6 weeks following the 2009 pH1N1 vaccination [30], the cumulative risk of GBS among the vaccinated and unvaccinated population at the end of the surveillance period (which correlated with the end of the pandemic and the end of administration of 2009 pH1N1 vaccines) was assessed using a survival analysis. The cumulative risk of GBS was significantly higher among the unvaccinated population than the vaccinated population (9.2 per million vs 6.6 per million persons; P = .012; Figure 3). There may indeed be an increased risk of GBS during the 6 weeks following vaccination, and evidence supports this assertion, but at the population level the survival analysis shows that the overall risk of GBS among those vaccinated was lower during the 2009 H1N1 pandemic [43]. Previously, Tam et al and Stowe et al suggested similar protective effect of influenza vaccinations, by way of preventing influenza infection itself, on GBS risk [23, 40]. Finally, 2 recent robust analyses, from Greene et al and Kwong et al [44, 45], assessed the association of GBS following influenza vaccines as well as following medically attended infections (specifically influenza in the Kwong et al study). In the Greene et al analysis, data on >9 million individuals from 10 US healthcare organizations was used to determine the observed vs expected odds of vaccination (with 2009 pH1N1 or 2010–2011 seasonal influenza vaccine) or infection occurring during the 6 weeks prior to GBS onset. This was a case-centered study design, which controls for time-varying confounders. The odds of vaccination prior to GBS onset adjusted for GBS onset date, age, sex, site, and infection status in the 6 weeks before GBS was 1.5 (95% CI, .6–4.0), whereas the odds of having a medically attended infection also adjusted for the same covariates and vaccination in the 6 weeks before GBS onset was 7.8 (95% CI, 3.6–16.6) [44]. The Kwong et al analysis used a self-controlled risk interval design and included vaccination from 1993 to 2011, from a population size of approximately 13 million. In this design, each individual serves as his or her own control, thus minimizing biases between vaccinated and unvaccinated comparisons. The risk of GBS was higher in the risk interval following vaccination exposure, with an attributable risk of 1.03 GBS cases per 1 million vaccinations. However, a much greater risk for GBS was found in the risk interval following medically attended influenza with an attributable risk of 17.2 cases per million influenza healthcare visits [45]. Both of these studies used individual-level information, looking at vaccination or medically attended infections during the same influenza seasons, and both provide compelling evidence that the risk of GBS following infections, including influenza, is far greater than the risk following influenza vaccination.
![Cumulative risk of Guillain-Barré syndrome (GBS) among the 2009 pH1N1 vaccinated and unvaccinated groups by day and all ages, Emerging Infections Program, United States, 15 October 2009–31 May 2010. Solid line is the cumulative rate of GBS per 1 million persons vaccinated with pH1N1; broken line is the cumulative rate of GBS per 1 million persons unvaccinated. Source: Reprinted with permission from Vellozzi et al [43].](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/cid/58/8/10.1093/cid/ciu005/2/m_ciu00503.jpeg?Expires=1716398874&Signature=xdUxvP4dii--IUL62MmvzuuDY5SNsSPLYJ4BrX0yK9P4pBhd65RgOiwyg1MJLRCBVQcAwTOCWdWZd55Efb0CF19QeXGTooBOFFSiRrPOWSvcP5rCzAuGqOLe5mby11ShY28IPFKhHXsXKX30SdYz1vFM7P4h92kGUkXWlrt7IevgWHgyzRir1esTmLtGmcUo4Ar0ZPz00r1IS-62pdQEoSx2I7iqo0uusTf3ZBw0o58vxH4q2aSdYuocmUN0lObOIBNTZUOa8ULq3Wq4yQyHDla2A6KUXF-n6ezQii9yo5jLQD2CPM7PBHWAnsGBAiFlHch0h1VWIWWecSnA0UCICw__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Cumulative risk of Guillain-Barré syndrome (GBS) among the 2009 pH1N1 vaccinated and unvaccinated groups by day and all ages, Emerging Infections Program, United States, 15 October 2009–31 May 2010. Solid line is the cumulative rate of GBS per 1 million persons vaccinated with pH1N1; broken line is the cumulative rate of GBS per 1 million persons unvaccinated. Source: Reprinted with permission from Vellozzi et al [43].
What have we learned over the last 35 years? First, increased risk of GBS has been found to be associated with both influenza infections and influenza vaccines. Second, many of the studies assessing the risk of GBS following influenza vaccines have not resulted in significant findings; however, most were not powered to do so; it is important to note that whenever a significant positive association has been reported, the increased risks of GBS following vaccination were well below the observed 8-fold risk following the 1976 swine-origin influenza vaccine and on average demonstrated an attributable risk about one-tenth of that for the 1976 swine-origin influenza vaccine. Third, the increased risk of GBS found following the 2009 pH1N1 vaccines, across several different studies, including a large international study, using different populations and study designs provides evidence in support of a causal association of GBS with influenza vaccination, although potential confounding due to influenza weakens the evidence somewhat. Perhaps during the 2009 H1N1 pandemic, the large population sizes under observation (EIP case finding) [29, 30] or the meta-analyses combining data from several sources (28 million people vaccinated contributed to the US meta-analysis) [33] provided sufficient power to detect a small increased risk for a very rare event.
Although monitoring for GBS following influenza vaccination remains important, we may have enough evidence to better understand the complex relationships between influenza, influenza vaccines, and the risk of GBS. Evidence supporting an increased risk of GBS during the 6 weeks following receipt of seasonal influenza vaccination is important for individual clinical decisions regarding vaccination and may be important for vaccine injury compensation program determinations. However, risk of GBS following vaccination should be weighed against the potential benefits of vaccination against influenza and reduction in influenza-related complications such as pneumonia, hospitalizations, or death. In summary, despite the small observed increased risk of GBS after influenza vaccination, evidence is growing in support of an apparent larger benefit of vaccination in regard to the overall risk of GBS in the context of population health [23, 40, 43].
Notes
Acknowledgments. The authors thank Oidda I. Museru, RN, MSN, MPH, at the National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention (CDC).
Disclaimer. The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the CDC.
Potential conflicts of interest. All authors: No reported conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.


{kind=link}
{kind=link}
{kind=link}
Comments