 PHATTHAYA AWISU/ ISTOCK/ GETTY IMAGES PLUS
PHATTHAYA AWISU/ ISTOCK/ GETTY IMAGES PLUS
Prevent Bleaching-Related Tooth Sensitivity
Relief is available for patients with painful sensitivity who desire a whiter, brighter smile.
Tooth sensitivity is the most common side effect of bleaching and may deter some patients from undergoing this cosmetic procedure. Bleaching-related tooth sensitivity is quite different from other causes of hypersensitivity, thus requiring an alternative treatment approach. This article focuses on the role of potassium nitrate. Other approaches, such as fluoride and amorphous calcium phosphate technologies, are available.
Pain Perception
The hydrodynamic theory is the widely accepted theory for dentin hypersensitivity.1 Fluid movement through the dentinal tubules activates mechanoreceptors in intratubular nerves and is perceived as pain.
Dentinal hypersensitivity is characterized by brief, sharp pain in response to thermal, tactile, chemical, evaporative, or osmotic stimuli that cannot be attributed to any other dental diseases.2
Dentin exposure can occur from bruxism, caries, recession, fractured teeth, gingivitis, periodontitis, acidic diet, recent dental procedures, and toothbrushing. Occlusal forces can also cause tooth mobility resulting in gingival recession and sensitivity or noncarious cervical lesions (NCCL) which become sensitive. Bruxism due to sleep apnea can result in NCCL or other tooth wear.
Treatment Modalities
Common treatment approaches for dentinal hypersensitivity include eliminating the causative stimuli, occluding the dentinal tubules, and reducing nerve transmission. For sensitivity related to restorative needs, a dentist may utilize resins or glass ionomer materials to seal tubules.
For teeth that do not require a restoration, topical applications of fluoride (gel, paste, or varnish) and oxalate salts may be used to occlude the dentin tubules and reduce fluid flow to pulp. Widely used in desensitizing toothpastes, 5% potassium nitrate works by depolarizing the nerve, thus reducing the nerve transmission.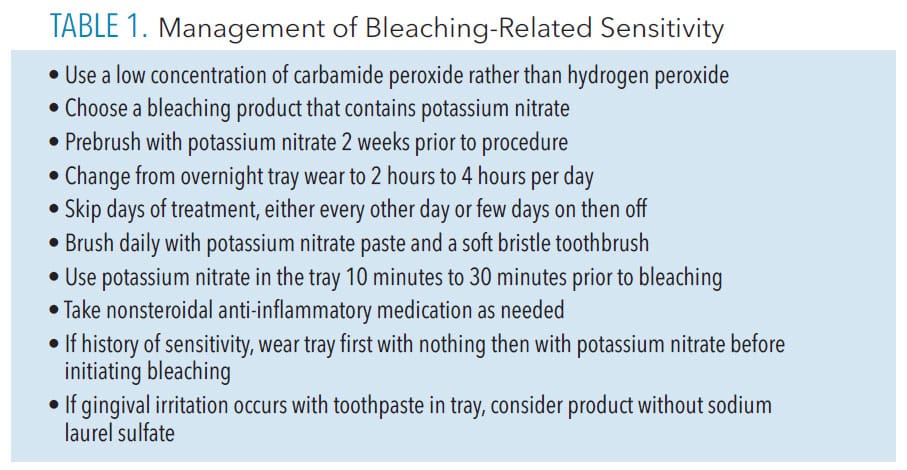
Whitening-Related Sensitivity
During tooth whitening, sensitivity occurs due to the easy passage of the peroxide molecule through intact enamel and dentin reaching the pulp in 5 minutes to 15 minutes.3 The tooth may not have recession, cracks, or restorations and still become sensitive.
This easy passage results in reversible pulpitis occurring a few days after starting the bleaching process.4 As bleaching sensitivity is not directly related to exposed dentinal tubules, different prevention approaches should be implemented (Table 1). These include but are not limited to: use of potassium nitrate, concentration of whitening material, type of bleaching agent utilized, length and frequency of treatment time, and toothpaste and toothbrush recommendations.
Potassium nitrate 5% is effective against tooth-bleaching sensitivity, as it reduces nerve pain by preventing repolarization of the nerve.5 Potassium nitrate also progresses through intact enamel and dentin to the pulp in 10 minutes to 30 minutes.3,6 It does not impact the efficacy of the bleaching process.
Potassium nitrate can be found in professional formulations and over-the-counter products as an active ingredient in desensitizing toothpastes. To ensure enough potassium nitrate is present in the dentifrice, the label must be examined. On the toothpaste box, ingredients are listed as either active or inactive. The active ingredients are listed from highest concentration ingredient to the lowest concentration. The patient needs a toothpaste with 5% potassium nitrate, which is the maximum concentration allowed by the United States Food and Drug Administration.3
When using a toothpaste with potassium nitrate, brushing generally takes 2 weeks to be effective due to the short duration time on the tooth. However, when potassium nitrate is placed directly in a bleaching tray, it can be effective in 10 minutes to 30 minutes.6–8 The potassium nitrate is used in place of the bleaching material whenever the sensitivity occurs.
Another option for a patient with a history of sensitive teeth is to start brushing with potassium nitrate 2 weeks before initiating bleaching. Bleaching should not be done the same day as a prophylaxis, which should be scheduled 2 weeks later due to the removal of the smear layer from the tooth or for gingival healing if necessary.
Anecdotally, women may be at risk for gingival irritation in response to the mint flavoring in many bleaching products, thus changing or eliminating the flavor should be considered.
If the patient continues to experience sensitivity, commercial versions of potassium nitrate are available. Additionally, patients with gingival irritation should look for a toothpaste without sodium lauryl sulfate, a common irritant.
Whitening Products
Traditional tray bleaching uses either carbamide peroxide or hydrogen peroxide. The most widely researched concentration is 10% carbamide peroxide, which contains approximately 3.5% hydrogen peroxide and 6.5% urea. Urea elevates the pH to above 8 within 5 minutes after initiation of bleaching. Most hydrogen peroxide products used in trays or over-the-counter products are at least 9%, which may result in more sensitivity. In general, the higher the concentration of peroxide in a product, the greater the chance of sensitivity.9
To reduce or prevent sensitivity during bleaching, the clinician may consider using a lower concentration of the bleaching agent, decreasing the time for each application, increasing the time between applications, and using a bleaching product that contains desensitizing agents.
Aggressive brushing may be a factor, thus patients should be educated about the proper use of a soft bristle toothbrush, advised to avoid highly abrasive toothpastes, and encouraged to use whitening products according to instructions. Patients may also want to eliminate or reduce highly acidic foods and drinks from their diets.
In-Office Bleaching
In-office bleaching causes more sensitivity due to the higher concentration of materials. The bleaching outcome of the tooth is the same whether in-office or at-home bleaching is used. If in-office is used to improve compliance, then sensitivity is addressed by either scheduling the multiple treatments spaced 1 week apart to allow the teeth to recover, or by following up one in-office treatment with tray bleaching to complete the process.
One in-office bleaching treatment is only successful in 24% of patients, and those patients would have a tooth shade lighter than A2 on a Vita shade guide.10 In-office bleaching often requires pain medication pre- and post-procedure.
Conclusion
Despite all these approaches, some patients will still experience sensitivity. However, approaching with realistic expectations and evaluating all the possible causes and corrections can provide most patients with a successful outcome from tray bleaching.
References
- Brännström M. The elicitation of pain in human dentine and pulp by chemical stimuli. Arch Oral Biol. 1962;7:59–62.
- Pashley DH, Tay F, Haywood V, Collins MA, Drisko CL (2008). Dentin hypersensitivity: Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. onsensus-based recommendations for the diagnosis and management of dentin hypersensitivity. Comp Contin Edu Dent. 2008;29:1–35.
- Kwon SR, Dawson DV, Schenck DM, Feigel J, Wertz PW. Spectrophotometric evaluation of potassium nitrate penetration into the pulp cavity. Oper Dent. 2015;40:614–621.
- Schulte JR, Morrissette DB, Gasior EJ, Czajewski MV. The effects of bleaching application time on the dental pulp. J Am Dent Assoc. 1994;125:1330–1335.
- Peacock JM, Orchardson R. Action potential conduction block of nerves in vitro by potassium citrate, potassium tartrate and potassium oxalate. J Clin Periodont. 1999;26:33–37.
- Kwon SF, Dawson DV, Wertz PW. Time course of potassium nitrate penetration into the pulp cavity and the effect of penetration levels on tooth whitening efficacy. J Esthet Restor Dent. 2016;28:S14–S22.
- Haywood VB, Caughman WF, Frazier KB, et al. Tray delivery of potassium nitrate-fluoride to reduce bleaching sensitivity. Quintessence Int. 2001;32:105–109.
- Haywood VB, Cordero R, Wright K, et al. Brushing with a potassium nitrate dentifrice to reduce bleaching sensitivity. J Clin Dent. 2005;16:17–22.
- Jorgensen MG, Carroll WB. Incidence of tooth sensitivity after home whitening treatment. J Am Dent Assoc. 2002;133:1076–1082.
- Gottardi MS, Brackett MG, Haywood VB. Number of in-office light-activated bleaching treatments needed to achieve patient satisfaction. Quintessence Int. 2006;37:115–120.
From Dimensions of Dental Hygiene. January 2023; 21(1)14-15.
